Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Diagnose and treat calcium blocker toxicity
Definition and mechanisms
- Calcium channel blockers (CCBs) are used to treat hypertension, supraventricular tachycardia, vasospasm, and migraine headaches
- Ingestion of excessive CCB agents is one of the most potentially lethal prescription drug overdoses
- Overdoses of immediate-release CCBs are characterized by rapid progression to hypotension, bradydysrhythmia, and cardiac arrest
- Overdoses of extended-release formulations result in delayed onset of dysrhythmias, shock, sudden cardiac collapse, and bowel ischemia
- Symptoms occur within six hours after ingestion, although some forms of medication do not start until after 24 hours
- Calcium channel blockers target the L-type voltage-gated calcium channels and these are predominant in the following sites and roles:
- Depolarization of the sinoatrial node (SA) and impulse propagation through the atrioventricular node (AV).
- Three main classes of CCBs:
- Phenylalkylamines (verapamil)
- Benzothiazepines (diltiazem)
- Dihydropyridines (nifedipine, amlodipine, felodipine, isradipine, nicardipine, nimodipine)
Signs and symptoms
- Dizziness
- Fatigue
- Nausea and vomiting
- Lightheadedness
- Altered mental status
- Coma
- Dyspnea
- Hypotension
- Bradycardia
- Hyperglycemia
- Metabolic acidosis
- Hypokalemia
- Hypocalcemia
- Pulmonary edema
- Renal failure
Diagnosis
- Hyperglycemia
- Blood gas: hyperlactatemia, metabolic acidosis, impaired oxygen delivery
- ECG:
- Bradycardia
- QT prolongation
- Bundle branch block
- First-degree atrioventricular block
- Junctional rhythms
- Sinus tachycardia (dihydropyridines)
- Echocardiography
- Chest X-ray: pulmonary edema
Complications
| Complications from toxicity | Complications from treatment |
|---|---|
| Refractory cardiogenic and distributive shock | Multiorgan failure from calciphylaxis with overaggressive calcium infusion |
| Acute Respiratory Distress Syndrome | Hypokalemia and Hypoglycemia |
| Severe hypoperfusion and resultant end-organ injury like ischemic bowel, myocardial infarction, acute tubular necrosis, limb necrosis | Acute Respiratory Distress Syndrome hypertriglyceridemia, pancreatitis, and fat overload syndrome with lipid emulsion therapy |
| Pulseless electrical activity with cardiac arrest (PEA) | Nausea, vomiting, ileus, and Hypokalemia with glucagon |
| Arterial and venous thrombosis and limb ischemia with interventions like ECMO |
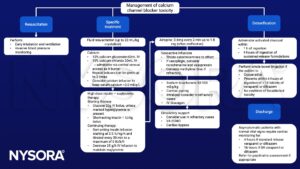
Management
Suggested reading
- Alshaya, O.A., Alhamed, A., Althewaibi, S., Fetyani, L., Alshehri, S., Alnashmi, F., Alharbi, S., Alrashed, M., Alqifari, S.F., Alshaya, A.I., 2022. Calcium Channel Blocker Toxicity: A Practical Approach. Journal of Multidisciplinary Healthcare Volume 15, 1851–1862.
- Jackson, R., Bellamy, M., 2015. Antihypertensive drugs. BJA Education 15, 280–285.
- St-Onge M, Dubé PA, Gosselin S, et al. Treatment for calcium channel blocker poisoning: a systematic review. Clin Toxicol (Phila). 2014;52(9):926-944.
- Kerns W 2nd. Management of beta-adrenergic blocker and calcium channel antagonist toxicity. Emerg Med Clin North Am. 2007;25(2):309-viii.