Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Diagnose and management of salicylate toxicity
Diagnosis and mechanisms
- Salicylate toxicity is the result of ingestion of, or (rarely) topical exposure to, chemicals metabolized to salicylate
- Poisoning may occur due to acute or chronic salicylate exposure
- Uncouple oxidative phosphorylation
- Interfere with the Krebs cycle
- Lead to accumulation of lactic acid & ketoacids
- Characterized by acid-base disturbances, electrolyte abnormalities, and central nervous system effects
- Unintentional salicylate toxicity is more common than intentional intoxication
- The most common source of salicylate poisoning is aspirin itself (acetylsalicylic acid) which is rapidly hydrolyzed to salicylate in the gastrointestinal tract, liver, and bloodstream
- Acute toxicity may occur after ingestion of a single dose of aspirin or the equivalent of >150 mg/kg or >6.5 g
- Chronic poisoning tends to occur as a result of repeated exposure to high-dose aspirin or equivalent (150 mg/kg/day), particularly in the setting of renal insufficiency
- Beware that many over-the-counter medications contain salicylates such as Pepto-Bismol, etheric oils, vapors, or analgesic ointments
- Herbs and spices such as ginger or mint also contain salicylates which can add to the drug burden
- Initially, symptoms such as tachypnea, lung crackles, and fever, often mimic a viral infection
- The classic triad of mild toxicity:
- Nausea
- Vomiting
- Tinnitus
Pathophysiology
Therapeutic levels of salicylates
- Irreversibly block COX-1 and modify COX-2 leading to a decrease in inflammation and platelet aggregation
Toxic levels of salicylates
- Stimulate the respiratory center causing hyperpnea
- Shift in metabolism to glycolysis for energy production → ↑ oxygen consumption and heat production → lactic acidosis
Signs and symptoms
| Nervous system | Tinnitus Listlessness Vertigo and incoordination Hallucinations Muscle rigidity Seizures Cerebral edema Coma |
| Gastro-intestinal | Nausea Vomiting |
| Respiratory | Hyperpnea Noncardiogenic pulmonary edema |
| Cardiac | Cardiovascular collapse |
| Metabolic | Fever Respiratory alkalosis Increased anion-gap metabolic acidosis (late sign) Hypernatremia due to fluid deficit Hypokalemia |
Diagnosis
- Arterial blood gases
- Serum electrolyte panel
- Serum salicylate level
- BUN and creatinine
- ECG
- Head CT scan
- EEG
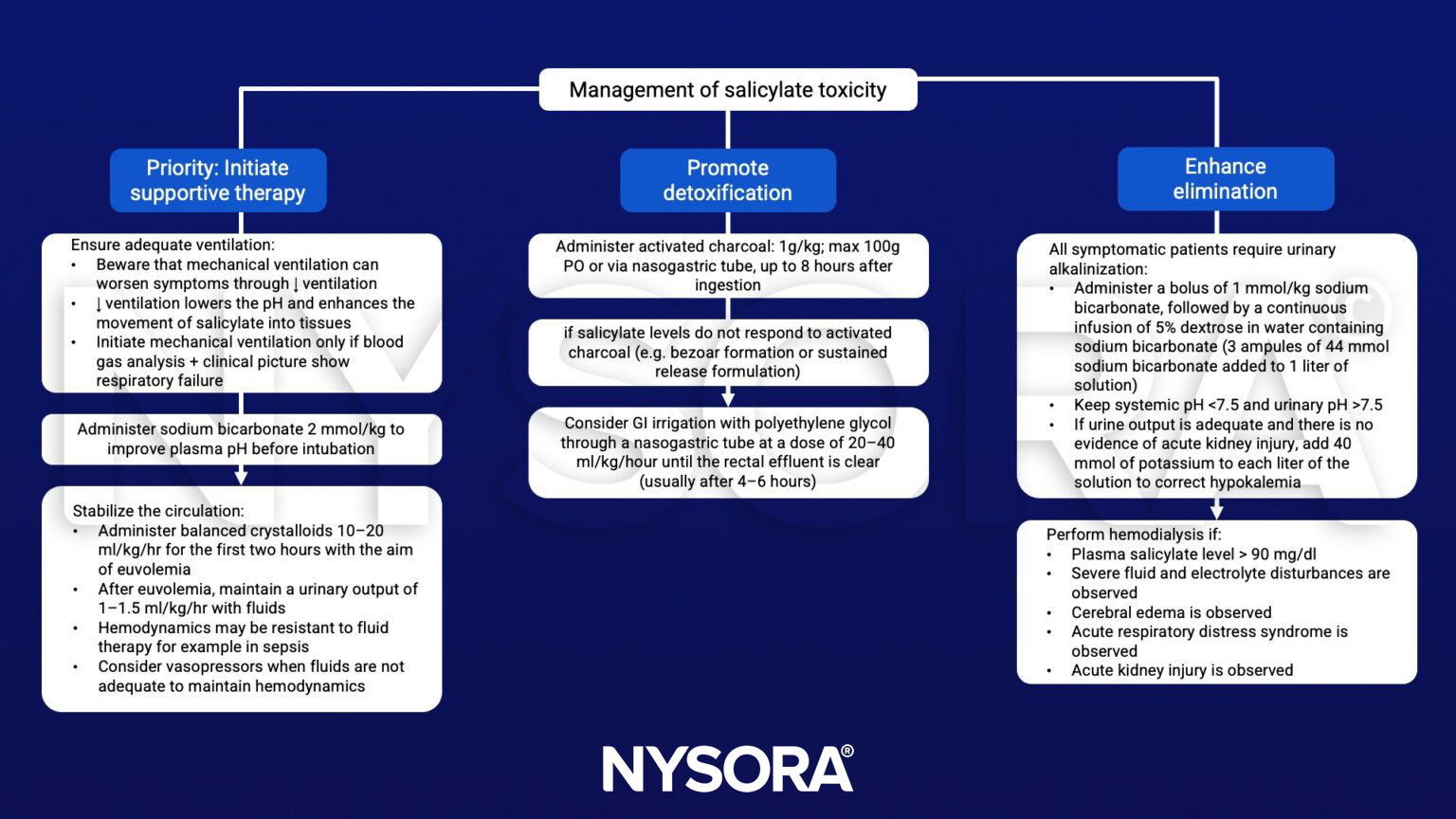
Management
Suggested reading
- Palmer BF, Clegg DJ. Salicylate Toxicity. N Engl J Med. 2020;382(26):2544-2555.