Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About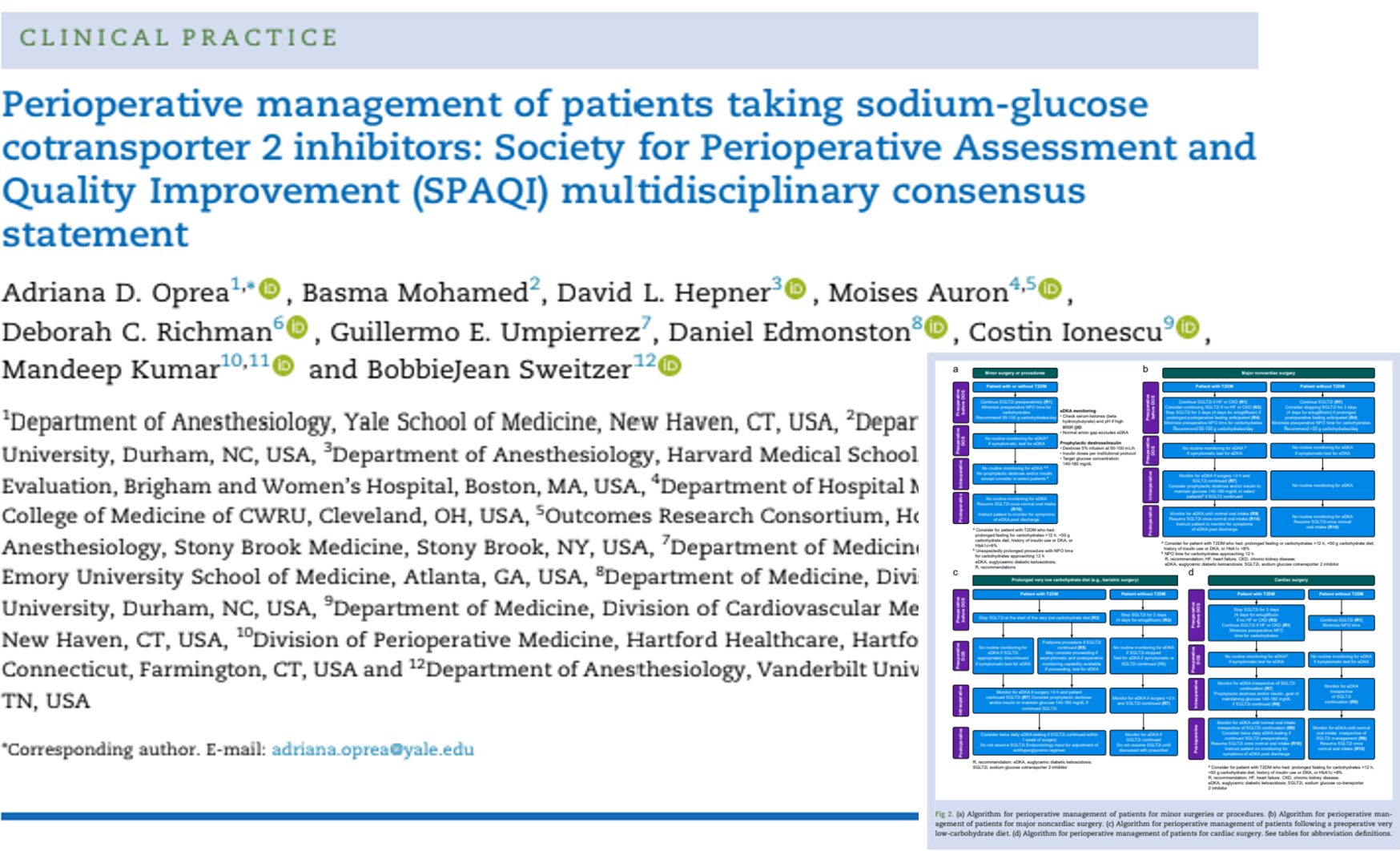

New international consensus reshapes perioperative management of SGLT2 inhibitors
The Society for Perioperative Assessment and Quality Improvement (SPAQI) has published a major multidisciplinary consensus statement that challenges the traditional “one-size-fits-all” strategy for perioperative management of sodium-glucose cotransporter 2 inhibitors (SGLT2 inhibitors).
Published in the British Journal of Anaesthesia, the consensus proposes an individualized, risk-based approach that balances the risk of euglycemic diabetic ketoacidosis (eDKA) against the increasingly recognized cardiovascular and renal benefits of continuing SGLT2 inhibitors in selected surgical patients.
As SGLT2 inhibitors are now routinely prescribed not only for type 2 diabetes but also for heart failure and chronic kidney disease, perioperative clinicians are caring for a rapidly growing number of patients receiving these medications.
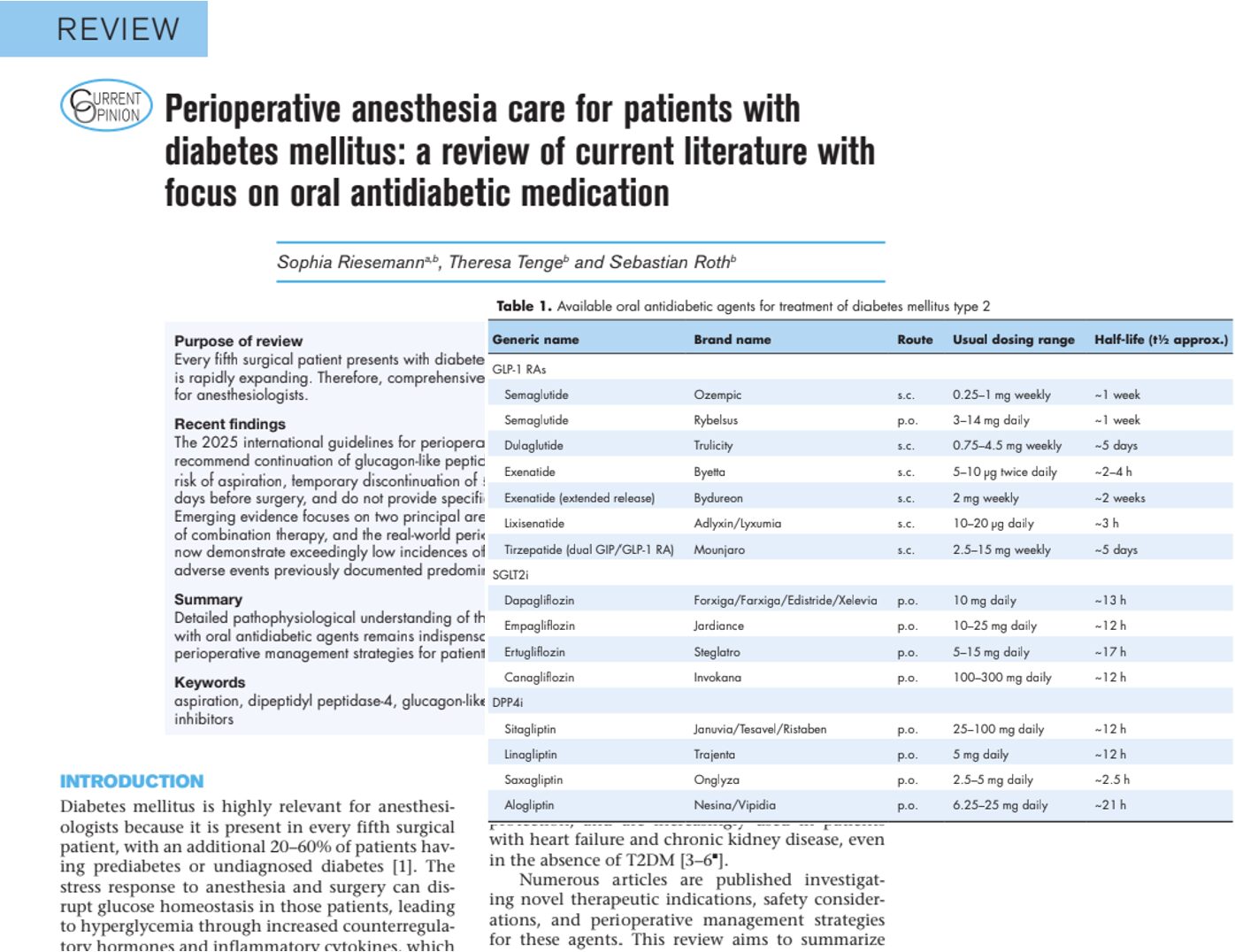
What are SGLT2 inhibitors?
SGLT2 inhibitors reduce renal glucose reabsorption in the proximal tubule, producing glucosuria while also promoting natriuresis and mild osmotic diuresis.
Common agents include:
- Empagliflozin (Jardiance)
- Dapagliflozin (Farxiga)
- Canagliflozin (Invokana)
- Ertugliflozin (Steglatro)
- Bexagliflozin (Brenzavvy)
- Sotagliflozin (Inpefa)
Although originally developed for glycemic control in type 2 diabetes, these medications now have established indications for:
- Heart failure with reduced ejection fraction
- Heart failure with preserved ejection fraction
- Chronic kidney disease
- Cardiovascular risk reduction in selected patients
These expanding indications have complicated perioperative decision-making because many patients taking SGLT2 inhibitors no longer have diabetes.
Why perioperative management remains controversial
Current FDA recommendations advise stopping most SGLT2 inhibitors three days before surgery (four days for ertugliflozin), regardless of the indication.
However, the SPAQI panel argues that this universal recommendation may unnecessarily interrupt therapies that protect against:
- Acute kidney injury
- Heart failure decompensation
- Major adverse cardiovascular events
- Mortality
Conversely, continuing therapy in inappropriate patients increases the risk of euglycemic diabetic ketoacidosis, a potentially life-threatening complication that may occur despite normal blood glucose concentrations.
What is euglycemic diabetic ketoacidosis?
Unlike classic diabetic ketoacidosis, patients with eDKA often have:
- Blood glucose below 200 mg/dL
- Elevated serum ketones
- Metabolic acidosis
- Increased anion gap
Because hyperglycemia is absent or mild, diagnosis may be delayed.
Typical symptoms include:
- Nausea
- Vomiting
- Abdominal pain
- Fatigue
- Tachypnoea
- Altered mental status
The consensus emphasizes that clinicians should maintain a high index of suspicion following surgery, especially in patients with diabetes who continue SGLT2 inhibitors.
Which patients are at highest risk?
Diabetes-related factors
- Type 2 diabetes
- Poor glycemic control (HbA1c >8%)
- Previous diabetic ketoacidosis
- Insulin therapy
- Reduction or omission of insulin
Dietary factors
- Ketogenic diets
- Very low-carbohydrate diets
- Bariatric surgery diets
- Prolonged fasting
- Dehydration
Surgical factors
- Cardiac surgery
- Major non-cardiac surgery
- Bariatric surgery
- Emergency surgery
- Prolonged postoperative fasting
Patients without diabetes who receive SGLT2 inhibitors for heart failure or chronic kidney disease appear to have a substantially lower risk of perioperative eDKA.
The biggest change: personalized perioperative management
Perhaps the most important message from the consensus is that perioperative management should depend on:
- Why the patient is taking the drug
- Whether diabetes is present
- Planned surgical procedure
- Expected fasting duration
- Presence of heart failure
- Presence of chronic kidney disease
- Planned dietary modifications
Rather than universally discontinuing therapy, the panel recommends individualized decision-making.
When should SGLT2 inhibitors usually be continued?
The consensus recommends continuing therapy in several situations.
Examples include:
- Minor surgical procedures
- Short ambulatory procedures
- Patients without diabetes undergoing most surgeries
- Patients with heart failure undergoing cardiac surgery
- Patients with chronic kidney disease undergoing many procedures
- Patients expected to resume carbohydrate intake promptly
These recommendations reflect the growing evidence supporting preservation of cardiovascular and renal benefits during the perioperative period.
When should therapy be stopped?
The panel recommends discontinuing SGLT2 inhibitors before:
- Major surgery with prolonged postoperative fasting
- Cardiac surgery in patients with diabetes but without heart failure or chronic kidney disease
- Bariatric surgery
- Initiation of prolonged ketogenic or very low-carbohydrate diets
Recommended discontinuation:
- Three days before surgery
- Four days for ertugliflozin
The medication should generally be restarted only after normal oral intake has resumed.
Cardiac surgery deserves special attention
Cardiac surgery carries one of the highest reported risks for postoperative eDKA.
Nevertheless, these patients may also derive the greatest benefit from continuing SGLT2 inhibitors because studies suggest reductions in:
- Acute kidney injury
- Myocardial injury
- Cardiovascular complications
The SPAQI panel therefore recommends:
- Continuing therapy in selected patients with diabetes plus heart failure or chronic kidney disease
- Intensive perioperative monitoring
- Early use of dextrose and insulin when appropriate
- Frequent postoperative assessment for ketoacidosis
This represents one of the most significant departures from previous guidance.
Bariatric surgery remains high risk
Patients undergoing bariatric surgery are unique because they often follow ketogenic or very low-carbohydrate diets for several weeks before surgery.
The combination of:
- Carbohydrate restriction
- Surgical stress
- Reduced caloric intake
- Continued SGLT2 inhibitor therapy
creates an ideal environment for ketosis and eDKA.
For this reason, the panel recommends stopping SGLT2 inhibitors at the beginning of the bariatric diet rather than immediately before surgery.
New recommendations for perioperative monitoring
Routine laboratory monitoring is unnecessary for every patient.
Instead, monitoring should focus on higher-risk individuals.
Recommended tests include:
- Serum β-hydroxybutyrate
- Blood gas analysis
- Serum bicarbonate
- Anion gap
- Blood glucose
A normal anion gap makes clinically significant eDKA unlikely, while an elevated anion gap should prompt ketone testing.
How does this differ from previous guidelines?
Earlier recommendations largely focused on preventing eDKA by routinely discontinuing therapy.
The SPAQI consensus instead considers:
- Diabetes status
- Surgical complexity
- Duration of fasting
- Cardiovascular indications
- Kidney disease
- Individual patient risk
This more nuanced framework acknowledges that withholding therapy may not always produce the best overall outcome.
Clinical implications
The consensus may influence several areas of perioperative practice.
Potential changes include:
- More individualized medication planning
- Greater collaboration between anesthesiologists, surgeons, endocrinologists, cardiologists and nephrologists
- Increased perioperative ketone monitoring
- Greater emphasis on carbohydrate intake and hydration
- Better preservation of heart failure and kidney disease therapies
The recommendations also reinforce the importance of educating patients about the symptoms of eDKA after discharge.
Bottom line
The 2026 SPAQI multidisciplinary consensus represents a significant evolution in perioperative care for patients taking SGLT2 inhibitors. Rather than recommending universal preoperative discontinuation, the guideline advocates a personalized strategy that weighs the risk of euglycemic diabetic ketoacidosis against the proven cardiovascular and renal benefits of these medications. By incorporating diabetes status, surgical complexity, anticipated fasting, and comorbid heart failure or chronic kidney disease into perioperative planning, clinicians can make more informed decisions that optimize both safety and long-term outcomes. While further prospective trials are needed, this consensus provides the most comprehensive, risk-stratified framework to date for managing SGLT2 inhibitors around surgery.
Reference: Oprea AD et al. Perioperative management of patients taking sodium-glucose cotransporter 2 inhibitors: Society for Perioperative Assessment and Quality Improvement (SPAQI) multidisciplinary consensus statement. Br J Anaesth. 2026;136:1776-1799.
Read more about recent evidence like this in NYSORA’s Anesthesia Assistant app. Simulate case, check dosages and search through NYSORA knowledge database!