Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About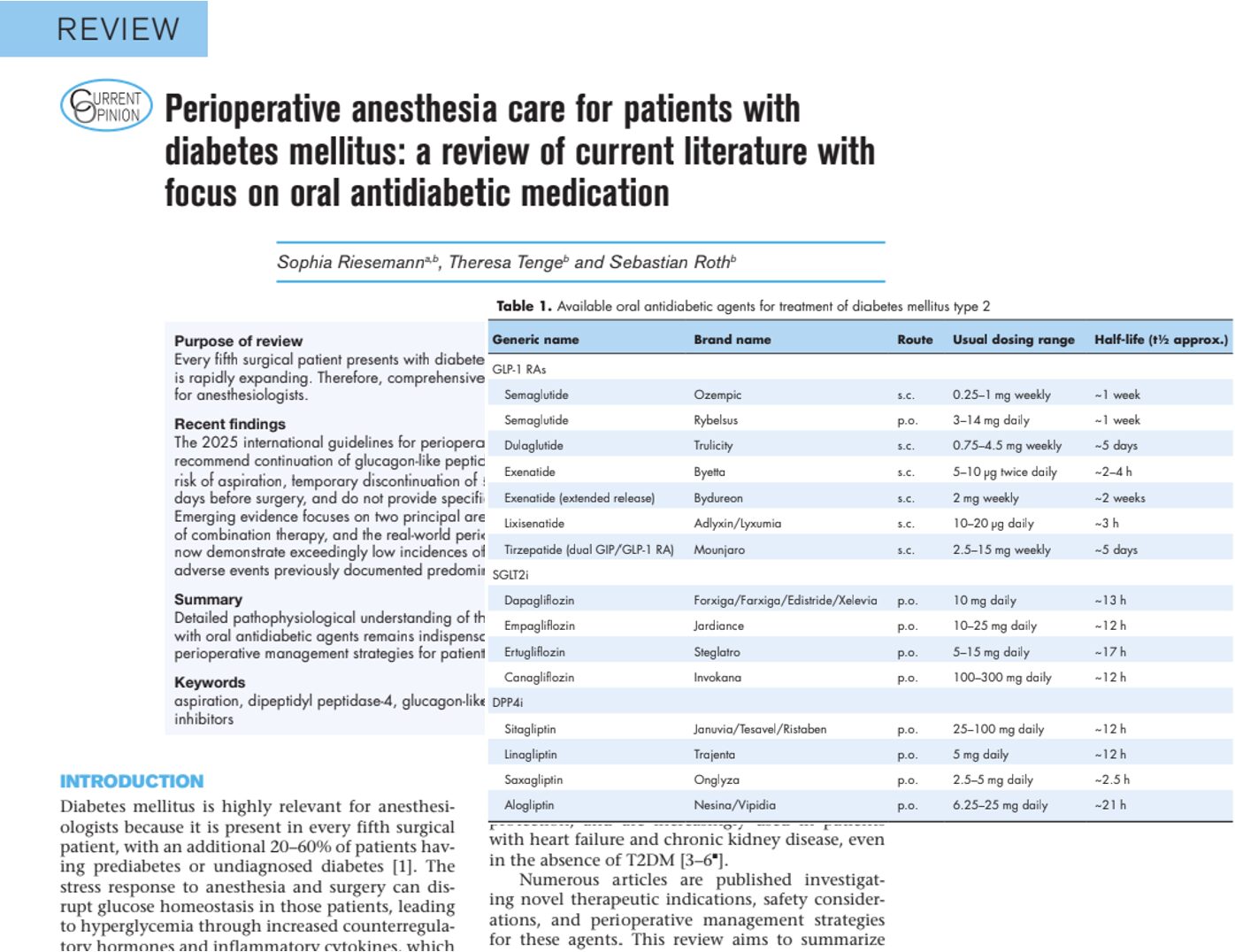





Introduction
Diabetes mellitus has become one of the most important chronic diseases encountered in surgical practice. According to recent literature, approximately one in five surgical patients has diabetes, while many additional patients present with prediabetes or undiagnosed disease.
The rapid expansion of newer antidiabetic therapies, including glucagon-like peptide-1 receptor agonists (GLP-1 RAs), sodium-glucose cotransporter-2 inhibitors (SGLT2 inhibitors), and dipeptidyl peptidase-4 inhibitors (DPP-4 inhibitors), has transformed diabetes management. However, these medications also create new challenges for anesthesiologists and perioperative clinicians.
A newly published review highlights evolving recommendations and emerging evidence regarding the perioperative management of these therapies.
Why diabetes matters during surgery
Surgery and anesthesia trigger a physiological stress response that can significantly disrupt glucose regulation.
This response increases:
- Catecholamine release
- Cortisol secretion
- Inflammatory cytokine production
- Hepatic glucose output
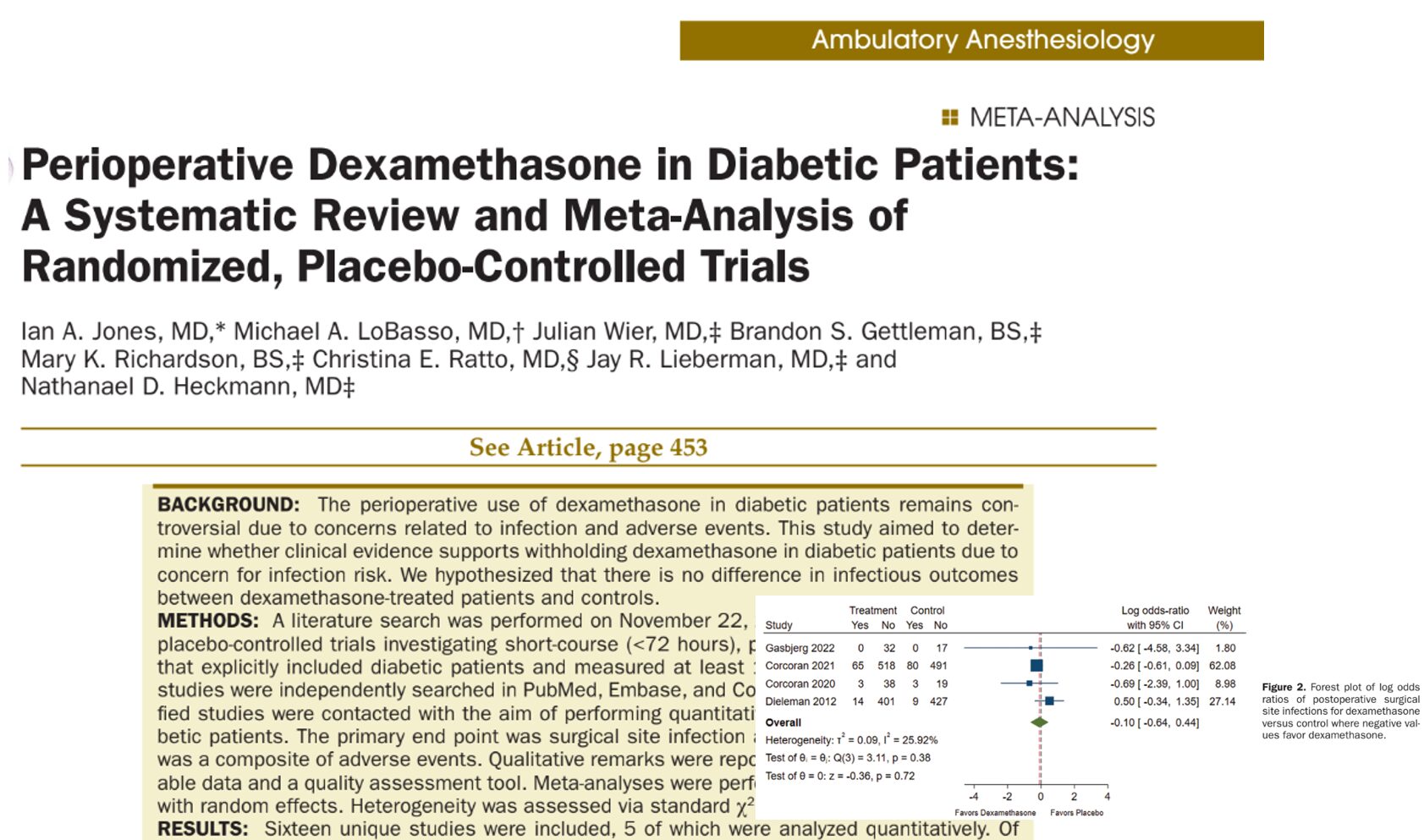
As a result, perioperative hyperglycemia may develop and contribute to:
- Surgical site infections
- Delayed wound healing
- Longer hospital stays
- Increased postoperative complications
- Higher mortality risk
Because of these risks, perioperative glucose management remains a cornerstone of surgical care.
Current recommendations for preoperative assessment
Recent guidance recommends that patients with diabetes undergo hemoglobin A1c (HbA1c) testing within three months before surgery.
Key recommendations
- Obtain HbA1c within 3 months of surgery.
- Consider postponing elective surgery when HbA1c exceeds 8%.
- Do not delay urgent or emergency surgery solely because of elevated HbA1c.
- Treat blood glucose levels above 180 mg/dL with insulin.
These measures help reduce perioperative complications and improve surgical outcomes.
Metformin: a changing perspective
For many years, clinicians frequently stopped metformin before surgery because of concerns regarding lactic acidosis.
However, more recent evidence challenges this practice.
How metformin works
Metformin:
- Suppresses hepatic gluconeogenesis
- Reduces glycogenolysis
- Improves insulin sensitivity
- Decreases intestinal glucose absorption
What the latest evidence shows
Large population studies have not demonstrated an increased risk of lactic acidosis among metformin users. As a result, recent cardiovascular and perioperative guidelines suggest that continuing metformin throughout the perioperative period is reasonable in many patients.
Clinical implications
Potential benefits of continuing metformin include:
- Improved glycemic stability
- Reduced glucose fluctuations
- Simpler medication management
- Lower risk of perioperative hyperglycemia
GLP-1 receptor agonists: the most debated drugs in anesthesia
Perhaps no drug class has generated more perioperative discussion than GLP-1 receptor agonists.
Popular medications include:
- Semaglutide (Ozempic, Rybelsus)
- Dulaglutide (Trulicity)
- Exenatide
- Tirzepatide (Mounjaro)
Why are these medications important?
GLP-1 receptor agonists provide:
- Excellent glucose control
- Significant weight loss
- Reduced cardiovascular risk
- Lower rates of major adverse cardiovascular events
Tirzepatide, which targets both GLP-1 and GIP receptors, has demonstrated even greater metabolic benefits in clinical trials.
The aspiration concern
The major perioperative concern involves delayed gastric emptying.
Because GLP-1 drugs slow gastric emptying, patients may retain stomach contents longer than expected. This raises theoretical concerns about:
- Regurgitation during anesthesia
- Pulmonary aspiration
- Aspiration pneumonia
Early recommendations suggested withholding these medications before surgery.
However, more recent evidence has altered that perspective.
New evidence on aspiration risk
A large 2025 meta-analysis involving more than 185,000 patients found:
- Increased residual gastric contents in GLP-1 users
- No statistically significant increase in pulmonary aspiration events
Another large study involving nearly 600,000 patients reported:
- Extremely low aspiration rates overall
- Lower observed aspiration rates among GLP-1 users compared with non-users
What guidelines now recommend
Most current international guidelines support:
- Continuing GLP-1 therapy in most patients
- Individualized risk assessment
- Use of gastric ultrasound when available
- Additional precautions in patients with severe gastrointestinal symptoms
Which patients may require extra caution?
Higher-risk patients include those with:
- Severe nausea
- Persistent vomiting
- Abdominal pain
- Gastroparesis
- Bowel dysmotility
- Parkinson disease
- Recent dose escalation of GLP-1 therapy
For these individuals, clinicians may consider:
- Extended fasting protocols.
- Gastric ultrasound evaluation.
- Delaying elective surgery when appropriate.
- Rapid-sequence induction techniques during anesthesia.
SGLT2 inhibitors: balancing benefits and risks
SGLT2 inhibitors have become increasingly important because they offer benefits extending beyond glucose control.
Common agents include:
- Empagliflozin
- Dapagliflozin
- Canagliflozin
- Ertugliflozin
Benefits of SGLT2 inhibitors
These medications provide:
- Improved glycemic control
- Cardiovascular protection
- Renal protection
- Heart failure benefits
- Reduced hospitalization rates in selected populations
The concern: euglycemic diabetic ketoacidosis
The principal perioperative concern is euglycemic diabetic ketoacidosis (eDKA).
Unlike traditional diabetic ketoacidosis, eDKA may occur despite relatively normal blood glucose levels.
Symptoms may include
- Nausea
- Vomiting
- Abdominal pain
- Fatigue
- Tachypnea
- Metabolic acidosis
Because blood glucose may appear relatively normal, diagnosis can be delayed.
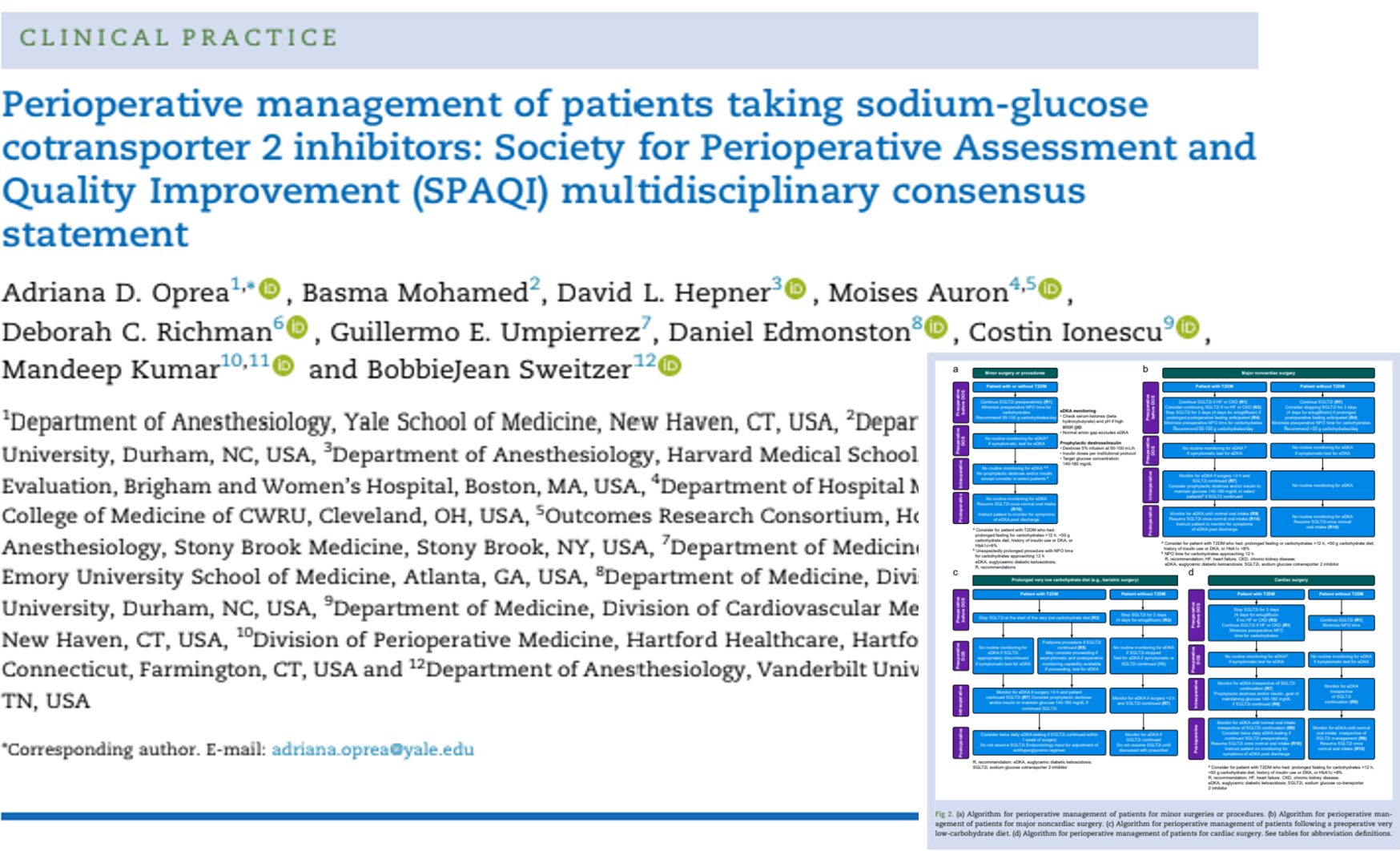
Current recommendations for SGLT2 inhibitors
Most contemporary guidelines recommend:
Before surgery
- Stop SGLT2 inhibitors approximately 3–4 days before surgery.
After surgery
- Restart once the patient:
- Is clinically stable
- Has resumed normal nutrition
- Shows no evidence of ketoacidosis
Emerging evidence challenges existing assumptions
Several large studies published recently have produced surprising findings.
Researchers observed:
- Lower postoperative mortality among SGLT2 inhibitor users
- Reduced acute kidney injury rates
- Potential organ-protective effects
- Mixed findings regarding ketoacidosis risk
One randomized pilot study in cardiac surgery patients even found:
- Less postoperative fluid accumulation
- Lower rates of acute kidney injury
- No observed ketoacidosis events
These findings suggest that future recommendations may become more individualized rather than universally stopping therapy.
DPP-4 inhibitors: the overlooked class
DPP-4 inhibitors often receive less attention than GLP-1 or SGLT2 therapies.
Common examples include:
- Sitagliptin
- Linagliptin
- Saxagliptin
- Alogliptin
Benefits
These medications:
- Improve glycemic control
- Have low hypoglycemia risk
- Are generally well tolerated
- Serve as alternatives when metformin cannot be used
Emerging research
New studies suggest DPP-4 inhibition may:
- Reduce systemic inflammation
- Improve endothelial function
- Stabilize vascular barriers
- Potentially protect organs during surgical stress
However, larger clinical trials are still needed.
Personalized perioperative care is the future
The review emphasizes that modern diabetes management requires individualized decision-making.
Rather than applying identical rules to every patient, clinicians should evaluate:
- Type of diabetes medication
- Surgical complexity
- Aspiration risk
- Renal function
- Cardiovascular disease
- Nutritional status
- Glycemic control
- Comorbid conditions
The goal is to preserve the proven benefits of these medications while minimizing perioperative risks.
Conclusion
The landscape of perioperative diabetes care is evolving rapidly. As the use of GLP-1 receptor agonists, SGLT2 inhibitors, and DPP-4 inhibitors continues to grow, anesthesiologists must remain informed about both the benefits and potential perioperative risks associated with these therapies.
Current evidence increasingly supports individualized, risk-based management rather than routine discontinuation of newer diabetes medications. While concerns such as aspiration risk and euglycemic ketoacidosis remain important, emerging data suggest that many of these drugs may also provide meaningful perioperative benefits, including cardiovascular and renal protection.
The overarching message from the latest review is clear: perioperative diabetes care should be personalized, evidence-based, and continuously updated as new research emerges.
Reference: Riesemann S et al. Perioperative anesthesia care for patients with diabetes mellitus: a review of current literature with focus on oral antidiabetic medication. Curr Opin Anaesthesiol. 2026;39:381-389.
Simulate your cases and access essential anesthesia knowledge, drug information, and perioperative guidance with the Anesthesia Assistant App.