Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About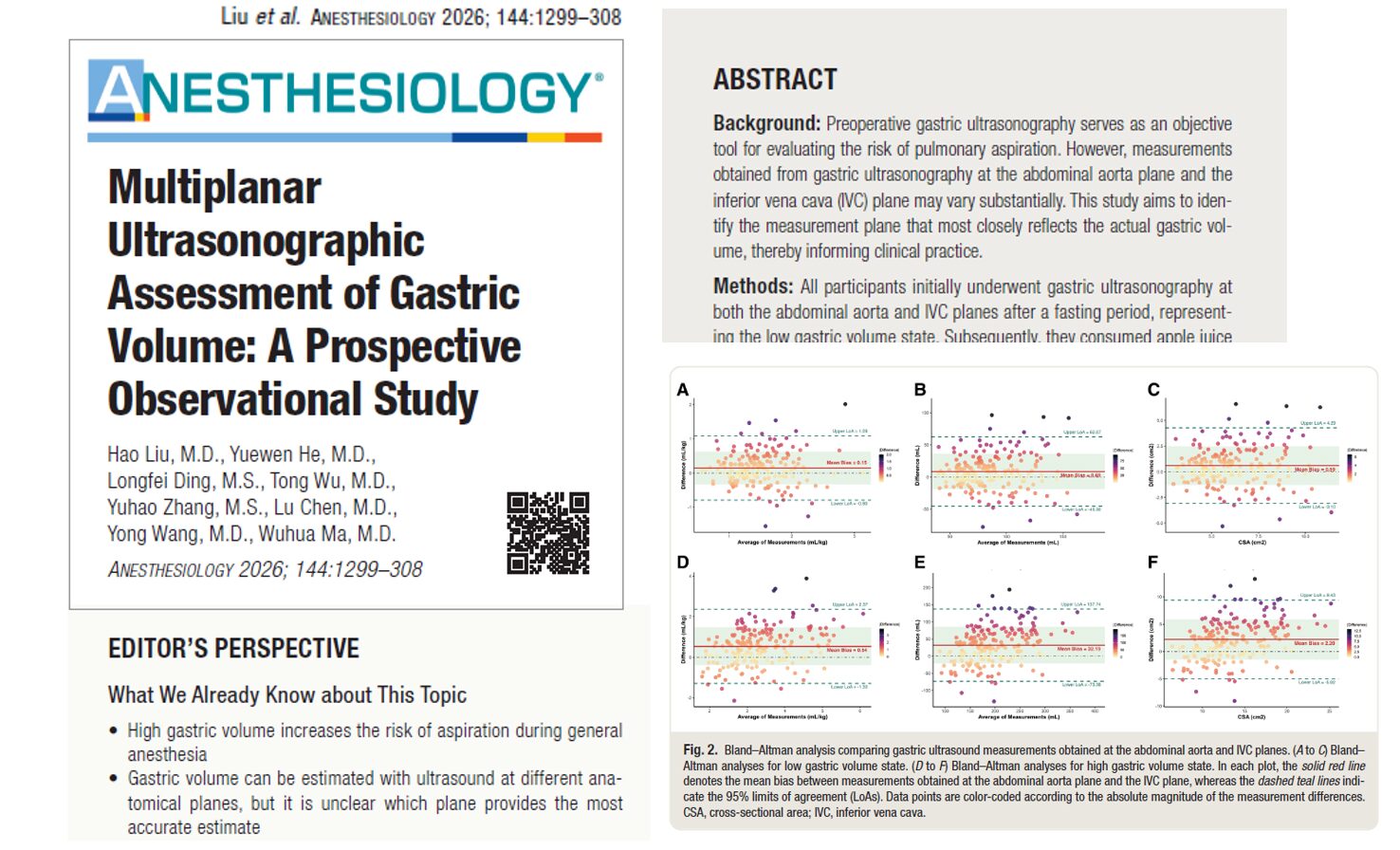

Pulmonary aspiration of gastric contents remains one of the most serious complications in anesthetic practice. Despite advances in fasting guidelines, airway management, and perioperative safety protocols, aspiration continues to contribute substantially to anesthesia-related morbidity and mortality.
Preoperative gastric ultrasonography has emerged as an important point-of-care tool for evaluating residual gastric contents and estimating aspiration risk. However, uncertainty remains regarding which ultrasound measurement plane provides the most accurate assessment of gastric volume.
A newly published prospective observational study by Liu et al. in Anesthesiology evaluated differences between gastric ultrasound measurements obtained at the abdominal aorta and inferior vena cava (IVC) planes. The findings suggest that neither plane is consistently superior, but selecting the higher-measured gastric volume may yield the most accurate estimate of actual gastric volume and aspiration risk.
What is gastric ultrasonography?
Gastric ultrasonography is a bedside imaging technique used to estimate gastric content volume and assess the risk of pulmonary aspiration before anesthesia.
The examination typically focuses on the gastric antrum while the patient is positioned in the right lateral decubitus position.
Clinicians commonly use two anatomical approaches:
- Abdominal aorta plane
- Inferior vena cava (IVC) plane
Both techniques utilize vascular landmarks to identify and measure the gastric antrum.
Why this study matters
Current gastric volume prediction models accept measurements from either the abdominal aorta or IVC planes.
Previous studies have used:
- Abdominal aorta plane only
- IVC plane only
- Either plane interchangeably
However, anatomical differences between these planes may influence gastric volume estimation and potentially affect aspiration risk assessment.
The investigators sought to determine:
- Whether the two measurement planes provide different gastric volume estimates
- Which plane most accurately reflects the actual gastric volume
- Whether one approach improves the detection of high aspiration risk patients
Study design
The researchers conducted a prospective observational study at Guangzhou University of Chinese Medicine.
The study enrolled healthy adult volunteers between July and August 2025.
Participant criteria included:
- Age greater than 18 years
- BMI ≤30 kg/m²
- ASA physical status I or II
- Ability to undergo gastric ultrasonography
A total of 202 volunteers were recruited.
Six participants were excluded because a clear visualization of the gastric antrum could not be obtained.
Final analysis included 196 participants.
Study protocol
The researchers evaluated gastric volume in two states.
- Low gastric volume state
Participants:
- Fasted for at least 8 hours
- Avoided water for 2 hours
- Underwent gastric ultrasonography at both measurement planes
- High gastric volume state
Participants then consumed apple juice at 2.3 mL/kg body weight
This amount corresponds to the currently accepted threshold associated with a full stomach and elevated aspiration risk.
Ultrasound measurements were repeated after ingestion.
Participant demographics
Baseline characteristics included:
- Median age: 23 years
- Median BMI: 20.97 kg/m²
- 48.5% male
- 51.5% female
- Median examination time: 2.5 minutes
Main findings
Significant differences between measurement planes
Researchers found statistically significant differences in abdominal aorta and IVC measurements between fasting and post-ingestion states.
After fluid ingestion:
Abdominal aorta plane
- Predicted gastric volume: 3.64 ± 1.11 mL/kg
- Mean gastric volume: 213.13 mL
IVC plane
- Predicted gastric volume: 3.11 ± 0.83 mL/kg
- Mean gastric volume: 180.94 mL
The abdominal aorta plane consistently produced larger gastric volume estimates.
The higher measured volume was most accurate
Investigators categorized measurements into:
- Abdominal aorta plane
- IVC plane
- Higher-measured gastric volume plane
- Lower-measured gastric volume plane
The most important finding was that the higher-measured gastric volume plane most closely matched the actual ingested volume.
Only this approach showed no statistically significant difference between predicted and actual gastric volume.
Key findings included:
- Mean bias: −4.27 mL
- P = 0.076 versus actual volume
- Smallest measurement error among all approaches
Aspiration risk detection
The researchers also evaluated how effectively each measurement strategy identified patients with high aspiration risk.
Predicted ingested volume detection rates:
- Higher-measured gastric volume plane: 45.41%
- Abdominal aorta plane: 37.25%
- IVC plane: 19.90%
- Lower-measured gastric volume plane: 12.25%
High gastric volume state detection rates
- Higher-measured gastric volume plane: 95.41%
- Abdominal aorta plane: 90.31%
- IVC plane: 81.63%
- Lower-measured gastric volume plane: 76.53%
Why the planes may differ
The authors propose an anatomical explanation.
The IVC plane is located closer to the pylorus, a region that is less distensible than the gastric antrum.
As gastric volume increases:
- Gastric expansion becomes more pronounced
- Distension varies by location
- Measurement discrepancies widen
This may explain why differences between planes were larger after fluid ingestion than during fasting.
Clinical implications
The findings may have important implications for perioperative practice.
Potential benefits include:
- Improved gastric volume estimation
- More accurate aspiration risk stratification
- Better perioperative decision-making
- Enhanced patient safety
- More individualized anesthesia planning
The authors recommend distinguishing between the abdominal aorta and IVC planes and using the higher measured gastric volume when applying current predictive models.
Limitations
The investigators acknowledged several limitations:
- Single-center study
- Relatively young and healthy participants
- BMI limited to ≤30 kg/m²
- Results may not generalize to all surgical populations
- Ultrasound examinations were performed by an experienced operator
- Acceptable limits of agreement for gastric ultrasound remain undefined
Additional studies are needed to validate these findings in broader patient populations.
Key takeaways
- Gastric ultrasound measurements differ significantly between the abdominal aorta and the IVC planes
- Measurement discrepancies increase as gastric volume rises
- Neither plane is consistently superior
- The higher measured gastric volume most closely reflects actual gastric volume
- Using the higher value may improve the aspiration risk assessment
- Current predictive models may benefit from incorporating measurement-plane differences
Future directions
Future research may explore:
- Development of plane-specific prediction models
- Validation in obese patients
- Evaluation in emergency surgery populations
- Application in patients with delayed gastric emptying
- Integration with artificial intelligence-assisted image analysis
- Multicenter validation studies
Conclusion
This prospective observational study provides important new evidence that the selection of the ultrasound measurement plane significantly influences gastric volume estimation.
Rather than relying exclusively on either the abdominal aorta or IVC plane, clinicians may improve the accuracy of aspiration risk assessment by evaluating both views and using the higher measured gastric volume when applying current prediction models.
As gastric ultrasonography becomes increasingly integrated into perioperative care, these findings may help refine risk stratification and improve patient safety during anesthesia. For more information, refer to the full article in Anesthesiology.
For more information, refer to the full article by Liu et al. in Anesthesiology.
Liu H, He Y, Ding L, et al. Multiplanar Ultrasonographic Assessment of Gastric Volume: A Prospective Observational Study. Anesthesiology. 2026;144(6):1299-1308.
Learn gastric ultrasound and more with NYSORA’s POCUS App!