Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Introduction
Traumatic rib fractures remain a significant cause of morbidity and mortality, particularly in older adults and polytrauma patients. Pain from rib fractures leads to impaired respiratory mechanics, reduced tidal volumes, and ineffective coughing, all of which predispose patients to complications such as atelectasis, pneumonia, and respiratory failure. Importantly, the use of systemic opioids—long considered the mainstay of analgesia—can further exacerbate respiratory depression, creating a challenging clinical paradox.
Thoracic epidural analgesia (TEA) has traditionally been regarded as the gold standard for pain control in patients with multiple rib fractures. However, TEA is not feasible in many trauma patients due to contraindications such as coagulopathy, spinal injuries, altered mental status, or hemodynamic instability. This gap in care has driven interest in alternative regional anesthesia techniques.
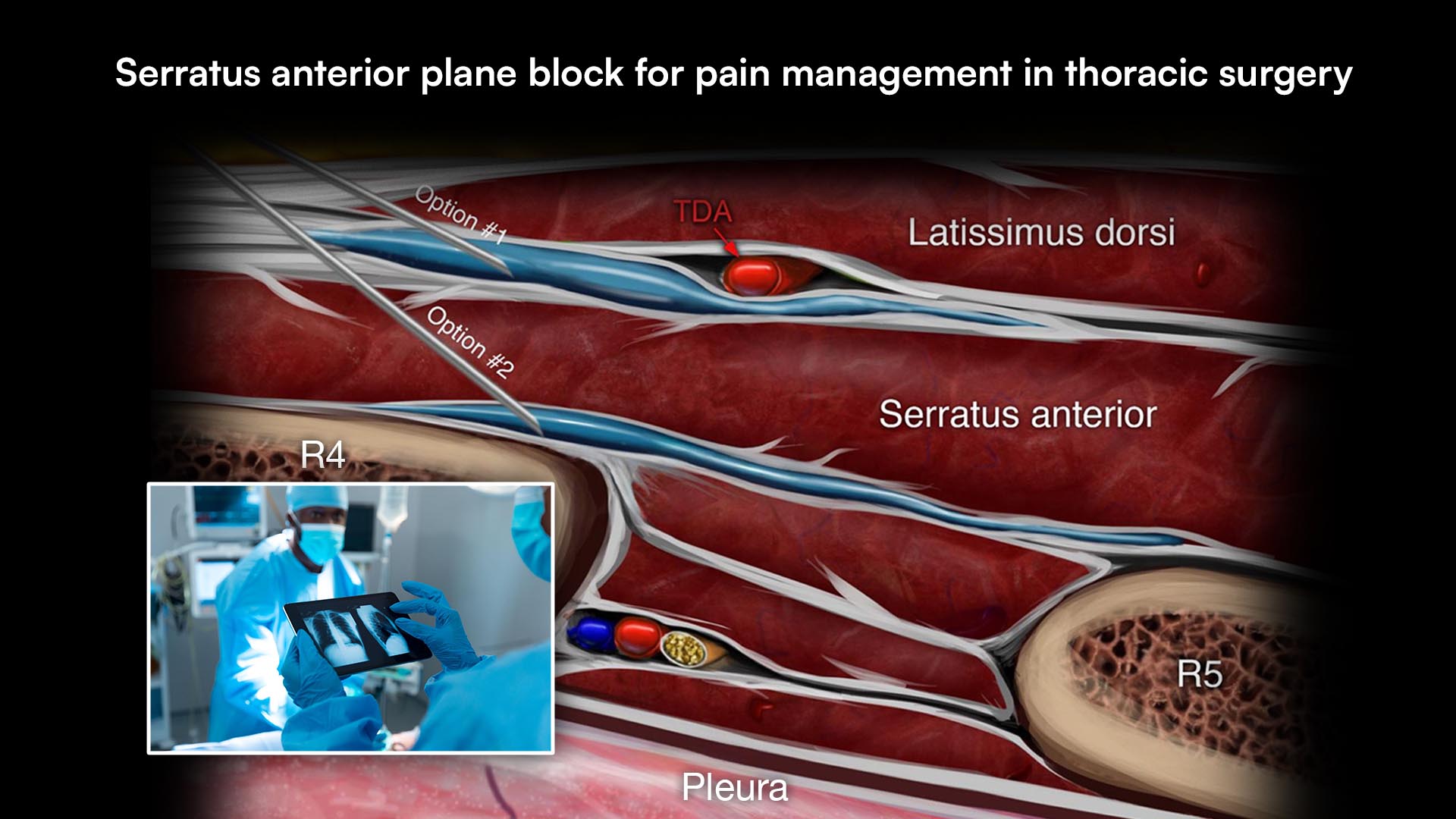
In recent years, thoracic fascial plane blocks—including erector spinae plane (ESP) block and serratus anterior plane block (SAPB)—have emerged as promising options. These techniques are technically simpler, safer in anticoagulated patients, and can be performed in a wider range of clinical settings. The scoping review by Niazi et al. provides a comprehensive evaluation of the current evidence supporting the use of these blocks in traumatic rib fractures.
Study objective and methods
The primary aim of this scoping review was to evaluate the effectiveness of thoracic fascial plane blocks in patients with multiple rib fractures, focusing on:
- Pain control
- Opioid consumption
- Respiratory function
Secondary objectives included assessing safety and comparing these techniques with traditional modalities such as TEA and paravertebral blocks (PVB).
Key methodological features
Comprehensive database search:
- PubMed
- Embase
- Cochrane databases
- Web of Science
- Scopus
- Google Scholar
- ClinicalTrials.gov
Timeframe:
- From database inception to October 2023
Inclusion criteria:
- Patients with unilateral or bilateral rib fractures
- Use of fascial plane blocks (ESP, SAPB, PEC, etc.)
- Reporting of pain or opioid outcomes
Study types included:
- Randomized controlled trials (RCTs)
- Cohort studies
- Case series and case reports
Total studies included:
- 64 full-text publications after screening over 5,000 citations
Key findings
- Analgesic efficacy
Both ESP and SAPB demonstrated consistent improvement in pain scores:
- Significant reduction in pain at rest and during movement
- Improved patient comfort and ability to participate in respiratory therapy
- Comparable analgesia to TEA in several RCTs
Notably, ESP provided similar pain relief to TEA but with improved hemodynamic stability.
- Opioid-sparing effects
A major advantage of fascial plane blocks is reduced opioid consumption:
- Lower morphine equivalent doses post-block
- Reduced need for IV PCA opioids
- Improved patient satisfaction
Some studies showed significant reductions in daily opioid use compared with systemic analgesia alone.
- Respiratory outcomes
Improved respiratory function was a key benefit:
- Increased inspiratory capacity
- Better incentive spirometry performance
- Reduced pain during coughing
However, evidence regarding reduction in major complications (e.g., pneumonia, ICU stay) remains limited and inconsistent.
- Comparison with traditional techniques
ESP vs TEA
- Comparable analgesia
- Better hemodynamic stability with ESP
- Fewer invasive requirements
SAPB vs PVB/TEA
- Similar pain control and respiratory outcomes
- Easier and faster to perform
- Better ultrasound visualization
ESP vs other blocks
- Comparable to a paravertebral block
- Superior to the intercostal nerve block in ED settings
- Safety profile
Fascial plane blocks demonstrated strong safety advantages:
- Superficial and compressible injection sites
- Lower risk in anticoagulated patients
- Minimal complications reported
These features make them particularly attractive in trauma populations.
Future research
Despite promising results, important gaps remain:
- Need for high-quality randomized controlled trials
- Direct comparisons between different fascial plane blocks
- Standardization of techniques and dosing
- Long-term outcomes (e.g., pulmonary complications, mortality)
Future studies should also explore optimal timing of block placement and multimodal analgesia strategies.
Clinical implications
The findings of this review have immediate relevance for clinicians:
- Fascial plane blocks can be used when TEA is contraindicated
- They are feasible in emergency departments, ICUs, and perioperative settings
- They support opioid-sparing strategies
- They may improve early mobilization and respiratory recovery
Importantly, these blocks expand access to regional anesthesia in trauma care.
Clinical pearls
- ESP and SAPB are the most studied and supported fascial plane blocks
- Both techniques provide effective analgesia for anterior, lateral, and posterior rib fractures
- ESP may offer broader dermatomal coverage due to paravertebral spread
- SAPB is quicker and technically easier to perform
- Early implementation may improve respiratory mechanics
Step-by-step: implementing a fascial plane block strategy
- Assess patient suitability
- Evaluate contraindications to TEA
- Review coagulation status
- Select the appropriate block
- ESP for posterior/multilevel fractures
- SAPB for lateral/anterior fractures
- Use ultrasound guidance
- Identify anatomical landmarks
- Ensure safe needle placement
- Administer local anesthetic
- Consider a continuous catheter for sustained analgesia
- Monitor outcomes
- Pain scores
- Opioid use
- Respiratory function
Conclusion
Thoracic fascial plane blocks represent a significant advancement in the management of traumatic rib fractures. The evidence synthesized in this scoping review demonstrates that techniques such as ESP and SAPB provide effective analgesia, reduce opioid requirements, and improve respiratory mechanics. While they may not fully replace thoracic epidurals, they offer a safer, more accessible alternative for many patients.
As trauma care continues to evolve, these blocks are poised to become a cornerstone of multimodal analgesia strategies. However, high-quality research is still needed to define their optimal role and long-term benefits.
Practical tip
Consider placing an ESP or SAPB within the first 24 hours of admission in patients with multiple rib fractures. Early analgesia can improve breathing mechanics, reduce opioid exposure, and potentially prevent downstream respiratory complications.
For more information, refer to the full article in RAPM.
Niazi AU, Solish M, Moorthy A, Niazi F, Abate AH, Devion C, Choi S. Use of fascial plane blocks for traumatic rib fractures: a scoping review. Reg Anesth Pain Med. 2026 Apr 2;51(4):414-428.
Get full access to fascial plane blocks (ESP, SAPB blocks) in the NYSORA Nerve Blocks app: technique walkthroughs, PRO tips, clinical videos, and more.