
- Learn
-
Apps
View all apps
Veterinary
 VetRA App
VetRA App

- Books
- Events
- News
- Partners
- About
- For Clinicians
 VetRA App
VetRA App
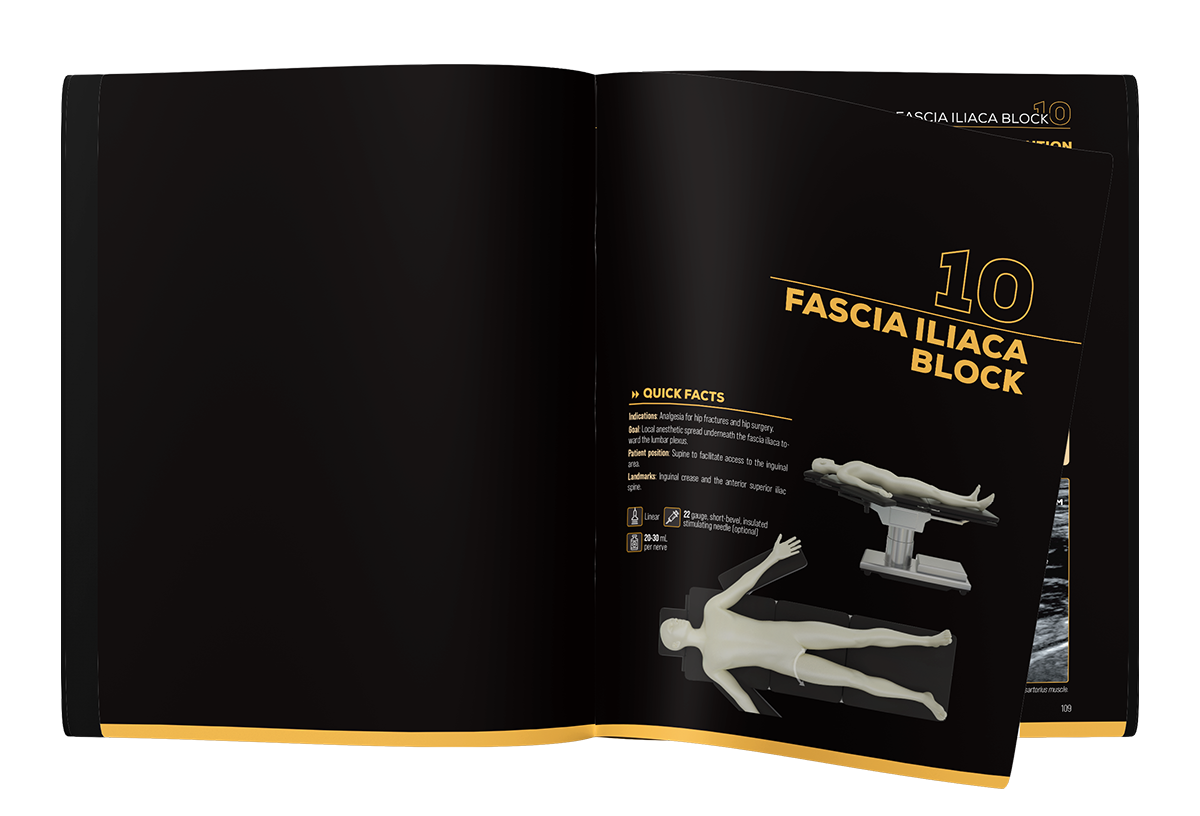
The ultimate guide to ultrasound-guided peripheral nerve blocks.




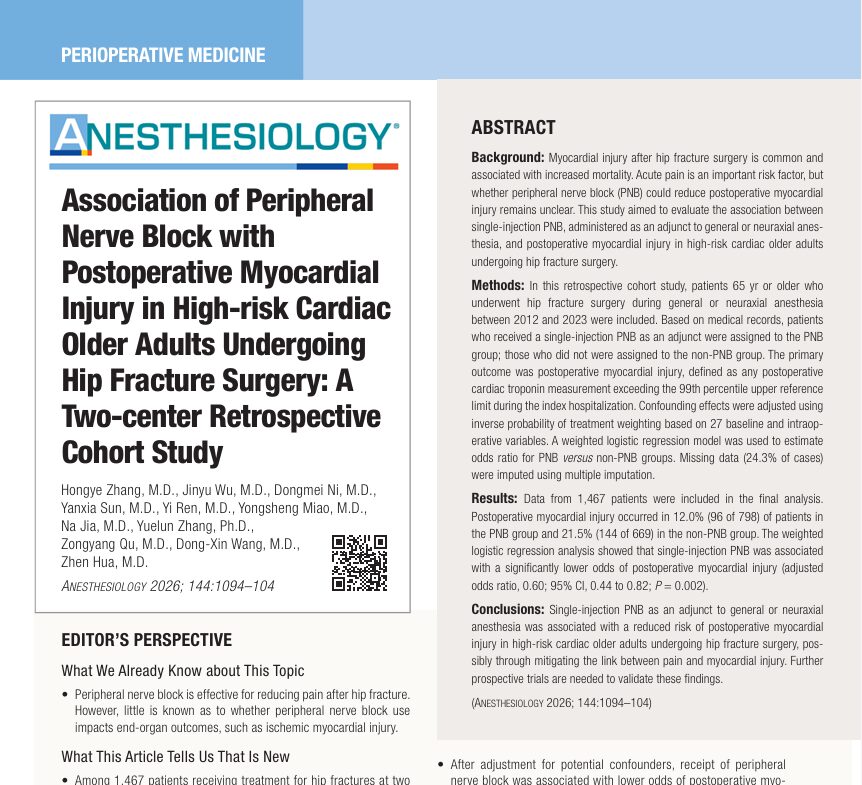
New study highlights protective cardiovascular effects of regional anesthesia A major new study published in Anesthesiology (2026) has revealed that peripheral nerve blocks (PNBs) may significantly reduce the risk of postoperative myocardial injury in older adults undergoing hip fracture surgery. This finding is particularly important because myocardial injury after noncardiac surgery (MINS) is a common and life-threatening complication, especially in elderly patients with pre-existing cardiovascular disease. The study analyzed 1,467 patients and provides strong evidence that optimizing perioperative analgesia may have cardioprotective effects beyond pain control. Understanding myocardial injury after hip fracture surgery What is myocardial injury? Myocardial injury refers to damage to cardiac muscle cells, typically identified by elevated cardiac troponin (cTn) levels above the 99th percentile upper reference limit. Indicates myocardial cell necrosis May occur with or without classic ischemic symptoms Strongly associated with increased mortality Why is it important? Occurs in 15–86% of hip fracture patients depending on population and monitoring Linked to: Increased 30-day mortality Higher 1-year mortality rates Prolonged hospitalization Hip fracture patients are especially vulnerable due to: Advanced age High prevalence of cardiovascular comorbidities Physiological stress from trauma and surgery Study overview: design and patient population Study design Two-center retrospective cohort study Conducted in Beijing, China Study period: 2012–2023 Participants 1,467 patients aged ≥ 65 years All underwent hip fracture surgery under: General anesthesia Neuraxial anesthesia Grouping Patients were divided into: PNB group (798 patients) Non-PNB group (669 patients) Nerve block techniques used Fascia iliaca compartment block (~70%) Femoral nerve block Lumbar plexus block Less common: Sciatic nerve block Pericapsular nerve group block Key findings: reduced risk of myocardial injury Primary outcome results Myocardial injury incidence: 12.0% with PNB 21.5% without PNB This represents a substantial reduction. Statistical analysis Adjusted odds ratio (OR): 0.60 95% confidence interval: 0.44–0.82 P = 0.002 (statistically significant) Interpretation […]
Effective postoperative pain control is a critical component of perioperative care in children undergoing cardiac surgery. Many pediatric cardiac procedures require a median sternotomy, a surgical approach that can produce significant nociceptive and neuropathic pain due to tissue dissection, rib retraction, sternal splitting, and placement of chest drains. Inadequate analgesia in this setting is not simply uncomfortable for the patient—it can contribute to physiologic instability and prolonged recovery. Pain that is poorly controlled after pediatric cardiac surgery has been associated with increased sympathetic activation, systemic hypertension, pulmonary hypertension, arrhythmias, and ventilator dyssynchrony. These complications may prolong mechanical ventilation and increase the length of stay in the intensive care unit (ICU). Furthermore, persistent poststernotomy pain and negative intensive care experiences may lead to chronic pain syndromes or long-term psychological stress responses in children. Historically, postoperative analgesia for pediatric cardiac surgery relied heavily on systemic opioids. While opioids remain effective analgesics, they are associated with well-recognized dose-dependent adverse effects. Respiratory depression, nausea, vomiting, ileus, and delayed extubation can complicate postoperative recovery. Prolonged opioid exposure may also lead to tolerance, dependence, or withdrawal symptoms in pediatric patients receiving continuous infusions for several days. Over the past decade, the increased availability of ultrasound-guided regional anesthesia has transformed perioperative pain management strategies. Fascial plane blocks in particular have gained attention because they provide targeted analgesia while maintaining a favorable safety profile in anticoagulated patients undergoing cardiopulmonary bypass. These techniques avoid the neuraxial and paravertebral spaces, reducing the risk of catastrophic hematoma formation. This growing interest has led clinicians to explore the use of fascial plane blocks as part of multimodal analgesia protocols for pediatric cardiac surgery. Recent studies suggest that these blocks may significantly reduce opioid requirements, improve postoperative recovery, and support enhanced recovery pathways. The challenge of poststernotomy pain in children Median sternotomy involves extensive […]
Available in paperback and Deluxe Edition—designed to refine technique, improve success, and patient safety.
The primary difference between the Nerve Block Manual and the Nerve Block Manual Deluxe lies in their presentation and design aesthetics.
The Nerve Block Manual offers detailed, step-by-step guidance on ultrasound-guided PNBs and fascial plane injection techniques, serving as an essential resource for medical professionals aiming to master these techniques.
Conversely, the Nerve Block Manual Deluxe is not just an instructional guide—it is truly a work of art. Printed on premium paper with superior bindings, every element of its design and layout is crafted with precision, resulting in an elegant and practical collector’s item. Moreover, the Deluxe Edition boasts a robust hardcover and is housed in a custom box adorned with raised plasticized color artwork. This deluxe edition is a treasure for practitioners, combining both top-notch content with a stunning design. Adding to its exclusivity, each copy is personally signed by Prof. Dr. Admir Hadzic himself, making it an invaluable addition to any medical professional’s collection.
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
