Learning objectives
- Diagnose and treat organophosphates toxicity
Definition and mechanisms
- Organophosphates toxicity often results from contact with organophosphate insecticides
- The majority of organophosphate toxicity occurs in farmers and people who work in agriculture
- The onset of symptoms is often within minutes and can persist for weeks
- Organophosphate pesticide exposure may occur through inhalation, ingestion, or dermal contact
- Organophosphate insecticides inhibit carboxyl ester hydrolases and mainly acetylcholinesterase (AChE), an essential enzyme in the breakdown of acetylcholine
- Resulting in the accumulation of acetylcholine and overstimulation of the nicotinic and muscarinic receptors
- Organophosphates stimulate both the sympathetic and parasympathetic nervous systems
Signs and symptoms
Mnemonics to remember the symptoms and the responsible receptor:
| For nicotinic signs of acetylcholinesterase inhibitor toxicity, think of the days of the week: | The more common mnemonic that captures the muscarinic effects of organophosphate poisonings is DUMBELS: | Additional symptoms |
|---|---|---|
| Monday = Mydriasis Tuesday = Tachycardia Wednesday = Weakness Thursday = Hypertension Friday = Fasciculations | D = Defecation/diaphoresis U = Urination M = Miosis B = Bronchospasm/bronchorrhea E = Emesis L = Lacrimation S = Salivation | Increased saliva and tear production Diarrhea Vomiting Small pupils Sweating Muscle tremors Anxiety Confusion Drowsiness Emotional lability Seizures Hallucinations Headaches |
Complications
- Neck flexions
- Weakness
- Decreased deep tendon reflexes
- Cranial nerve abnormalities
- Proximal muscle weakness
- Respiratory insufficiency
- Neuropathy
- Neuropsychiatric deficits:
- Confusion
- Memory impairment
- Lethargy
- Psychosis
- Irritability
- Parkinson like symptoms
Diagnosis
- Based on clinical suspicion
- Some organophosphates have a distinct garlic or petroleum odor
- Measurement of AChe in red blood cells
- Complete blood count
- Serum glucose levels
- Troponin levels
- Liver and renal function tests
- Arterial blood gas
- ECG
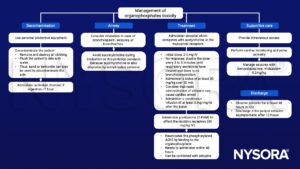
Management
Suggested reading
- Ward C, Sair M. 2010. Oral poisoning: an update. Continuing Education in Anaesthesia Critical Care & Pain. 10;1: 6-11.
- Geoghegan, J., Tong, J.L., 2006. Chemical warfare agents. Continuing Education in Anaesthesia Critical Care & Pain 6, 230–234.
Clinical updates
Nendumba et al. (Clinical Toxicology, 2025) report that intravenous lipid emulsion (ILE) therapy has emerging but limited evidence as an adjunctive treatment in severe organophosphate poisoning, based on animal studies, small clinical series, and case reports. While proposed benefits include lipid sink/shuttle effects and cardiotonic mitochondrial support, no mortality benefit has been demonstrated, and evidence quality remains low. ILE should therefore be viewed as a second-line or rescue therapy in refractory, life-threatening cases, without replacing standard management with atropine, oximes, benzodiazepines, and supportive care.
- Read more about this study HERE.