Learning objectives
- Defining, diagnosing, and managing hyponatremia
Definition
- Hyponatremia is defined as:
- Mild: a serum sodium concentration between 130-135 mmol/l
- Moderate: a serum sodium concentration between 125-129 mmol/l
- Severe at a serum sodium concentration <125 mmol/l
- Hyponatremia is acute if it is documented to exist <48 hours and chronic if it is documented to exist for at least 48 hours
- If unsure, consider chronic hyponatremia unless there is clinical or anamnestic evidence of the contrary
Signs and symptoms
- Moderate symptoms
- Nausea without vomiting
- Confusion
- Headache
- Severe symptoms
- Vomiting
- Cardiorespiratory distress
- Somnolence
- Seizures
- Coma
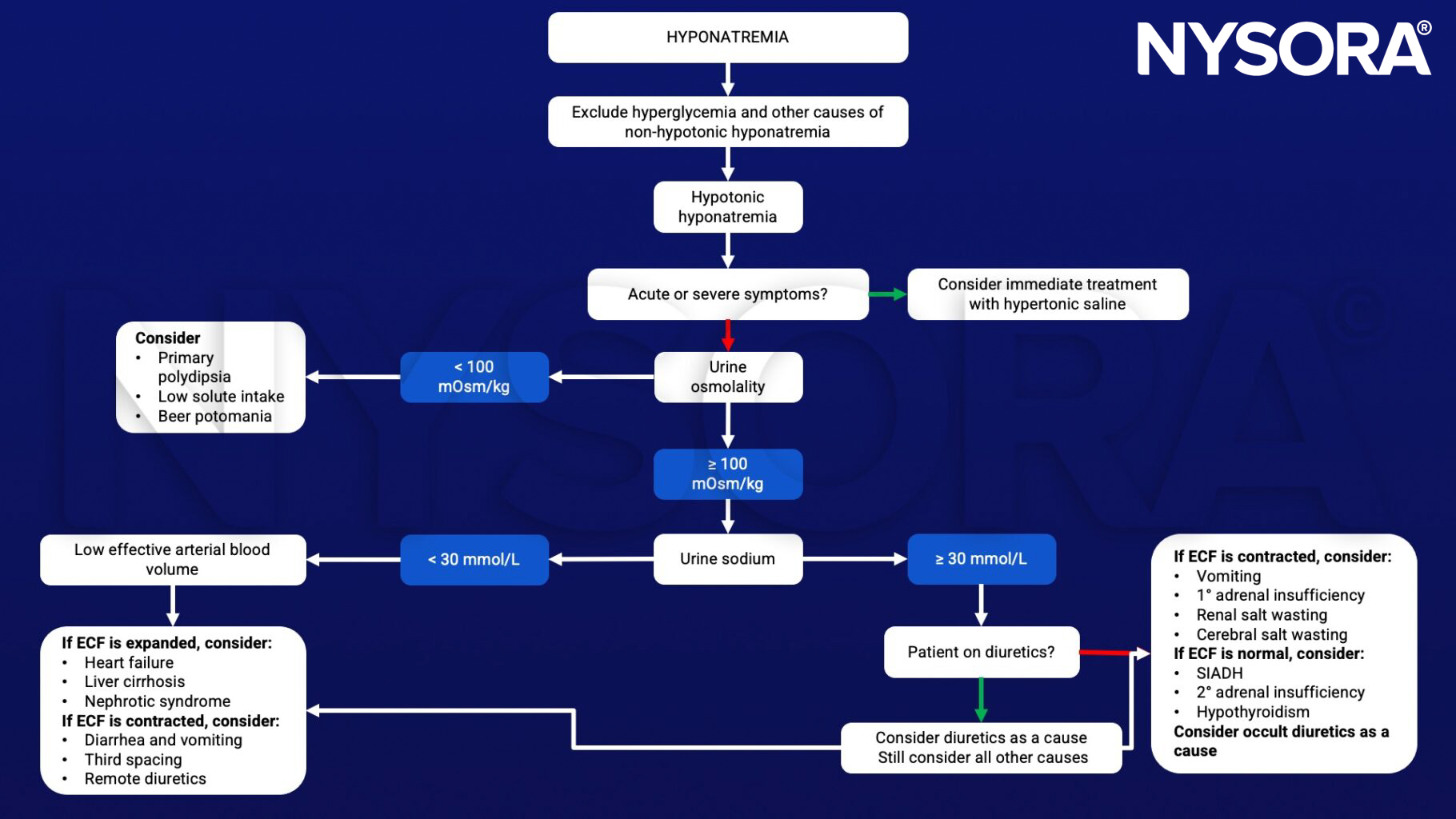
Differential diagnosis
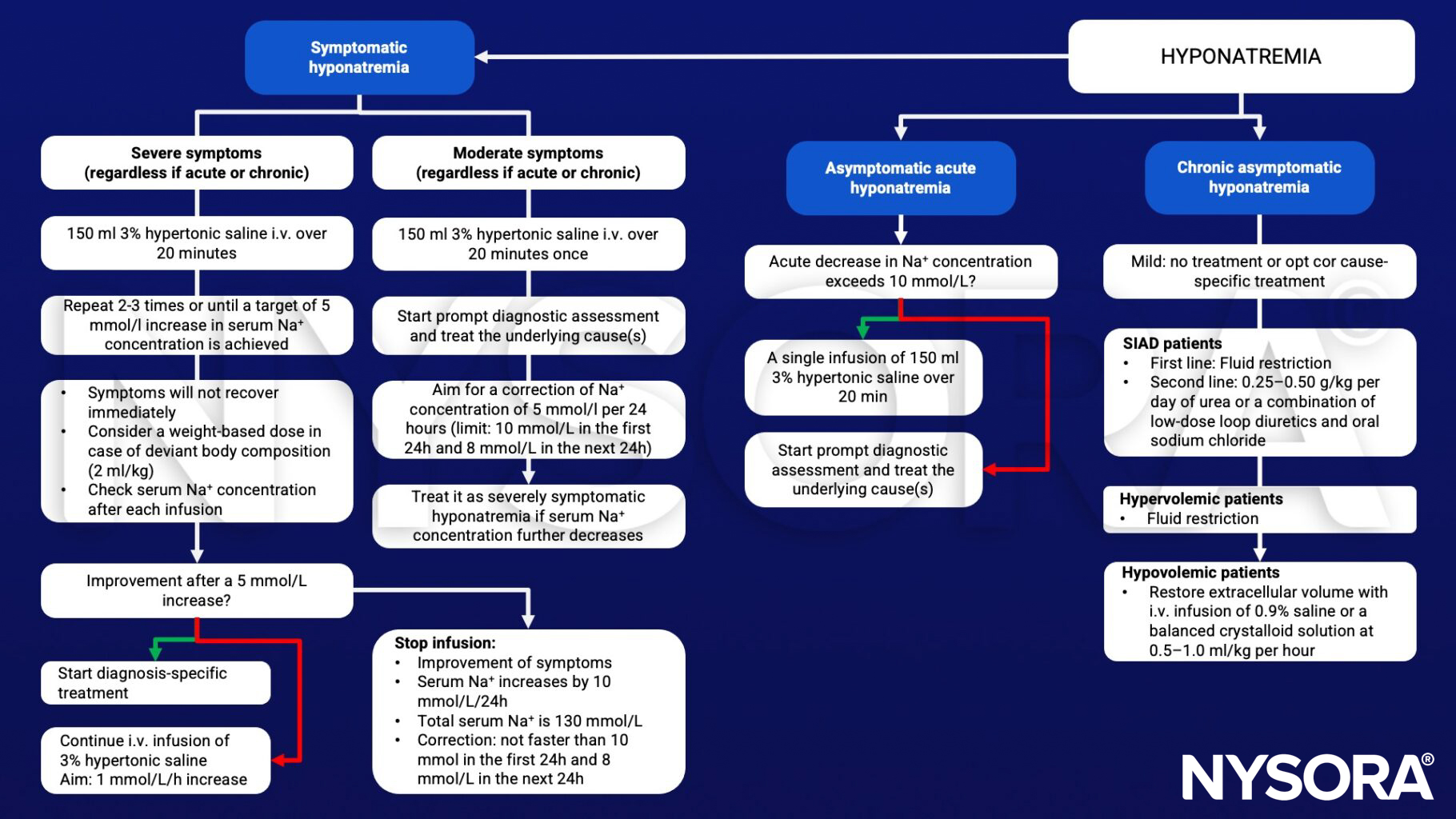
Management
Suggested reading
- Spasovski G, Vanholder R, Allolio B, et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia [published correction appears in Nephrol Dial Transplant. 2014 Jun;40(6):924]. Nephrol Dial Transplant. 2014;29 Suppl 2:i1-i39.
- Hoorn EJ, Zietse R. Diagnosis and Treatment of Hyponatremia: Compilation of the Guidelines. J Am Soc Nephrol. 2017;28(5):1340-1349.
Clinical updates
Fielding-Singh et al. (Anesthesiology, 2025) highlight that hyponatremia is common in patients on maintenance hemodialysis due to fluid retention and free water intake, and requires cautious perioperative management. The review emphasizes avoiding rapid sodium correction to prevent osmotic demyelination syndrome, particularly in chronically hyponatremic patients, and recommends individualized fluid planning and close electrolyte monitoring before and after surgery.
- Read more about this study HERE.
Sherman et al. (Current Opinion in Anaesthesiology, 2025) describe that hyponatremia is a common and prognostically significant feature in patients with advanced cirrhosis and hepatorenal syndrome (HRS), reflecting severe circulatory dysfunction and non-osmotic vasopressin release. The updated ICA–ADQI framework emphasizes early identification of HRS-AKI using KDIGO criteria and prompt initiation of albumin plus vasoconstrictor therapy, while avoiding rapid sodium correction to prevent neurologic complications. These evolving strategies aim to stabilize renal function, manage dilutional hyponatremia safely, and bridge patients to liver transplantation.
- Read more about this study HERE.
Lundblad et al. (British Journal of Anaesthesia, 2025) demonstrated in a prospective study of 365 infants undergoing surgery that intraoperative use of a 1% glucose-balanced electrolyte solution maintained stable sodium levels with only a small, clinically insignificant increase in mild hyponatremia. No cases of severe hyponatremia or associated complications were observed. These findings support the use of isotonic, low-glucose balanced fluids over hypotonic solutions to reduce the risk of perioperative hyponatremia in infants.
- Read more about this study HERE.