Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About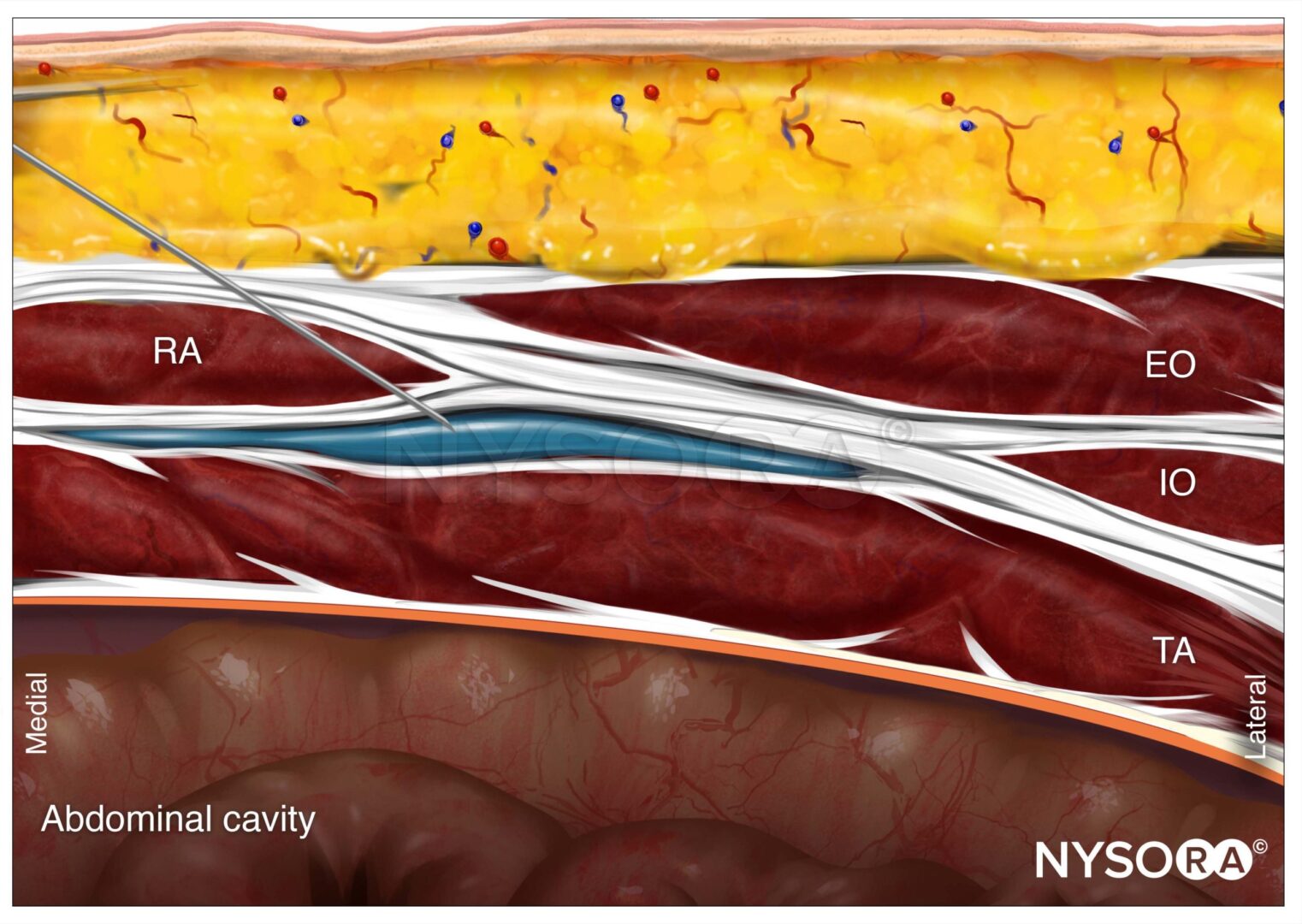
INTRODUCTION
Ultrasound-guided transversus abdominis plane (TAP) nerve block has become a common analgesic method after surgery involving the abdominal wall. Because TAP block is limited to somatic anesthesia of the abdominal wall and highly dependent on interfascial spread, various newer techniques have been proposed to enhance analgesia, either in addition to TAP nerve block or as a single modality. In particular, variants of quadratus lumborum nerve blocks (QLBs) have been proposed as more consistent methods with an aim to accomplish somatic as well as visceral analgesia of the abdomen. The present evidence, mainly case reports, suggests that different variants of QLB have different analgesic effects and mechanisms of action, although this has not been formally validated. In particular, transmuscular QLB and the so-called QLB2 may result in wider and longer sensory block compared to TAP nerve block (T4–L1 for QL nerve block vs. T6–T12 for the TAP nerve blocks) (Figures 1 and 2). This chapter focuses on underlying principles for TAP block and the newer QLB techniques, with an understanding that the information about the latter is based on sparse evidence of limited quality as outcome-based studies are not yet available.
FIGURE 1. The transverse abdominis plane (TAP) and quadratus lumborum 1 (QL1) nerve blocks anterior view. Injection of 20 mL of contrast in the TAP nerve block resulted in the posterolateral spread from the 12th rib to the iliac crest. The QL1 nerve block after injection of 20 mL of contrast resulted in the spread of the contrast toward the transverse process cephalad alongside the thoracolumbar fascia to the 11th and 10th intercostal spaces.
FIGURE 2. Transverse abdominis plane (TAP) and quadratus lumborum 1 (QL1) nerve blocks: posterior view. Injection of 20 mL of contrast in the TAP nerve block resulted in the posterolateral spread from the 12th rib to the iliac crest. After injection of 20 mL of contrast, the QL1 nerve block resulted in the spread of the contrast toward the transverse process cephalad alongside the thoracolumbar fascia to the 11th and 10th intercostal spaces.
ANATOMY
The transversus abdominis plane is the fascial plane superficial to the transversus abdominis muscle, the innermost muscular layer of the anterolateral abdominal wall. The upper fibrous anterior part of the muscle lies posterior to the rectus abdominis muscle and reaches the xiphoid process. The posterior aponeuroses of the transversus abdominis and internal oblique muscles fuse and attach to the thoracolumbar fascia (TLF). In the TAP, the intercostal, subcostal, and L1 segmental nerves communicate to form the upper and lower TAP plexuses, which innervate the anterolateral abdominal wall, including the parietal peritoneum. Therefore, TAP block requires anesthesia of the upper (also known as the subcostal or intercostal) TAP plexus, as well as the lower TAP plexus, located in the vicinity of the deep circumflex iliac artery.
The subcostal approach to the TAP nerve block ideally anesthetizes the intercostal nerves T6–T9 between the rectus abdominis sheath and the transversus abdominis muscle. The lateral TAP nerve block in the midaxillary line between the thoracic cage and iliac crest as well as between the internal oblique and transversus abdominis muscles ideally should reach intercostal nerves T10– T11 and the subcostal nerve T12. Of note, the umbilicus is innervated by intercostal nerve T10. The L1 segmental nerves in the TAP are not covered by the lateral TAP nerve block and require an anterior TAP nerve block medial to the anterior superior iliac spine. A posterior approach to nerve block the TAP plexuses via the triangle of Petit has also been described. TAP nerve blocks provide somatic analgesia of the abdominal wall including the parietal peritoneum.
The quadratus lumborum (QL) muscle lies in the posterior abdominal wall dorsolateral to the psoas major muscle (Figure 3). The QL muscle originates from the posterior part of the iliac crest and the iliolumbar ligament and inserts on the 12th rib and the transverse processes of vertebrae L1–L5. The QL muscle assists in lateral flexion of the lumbar spine.
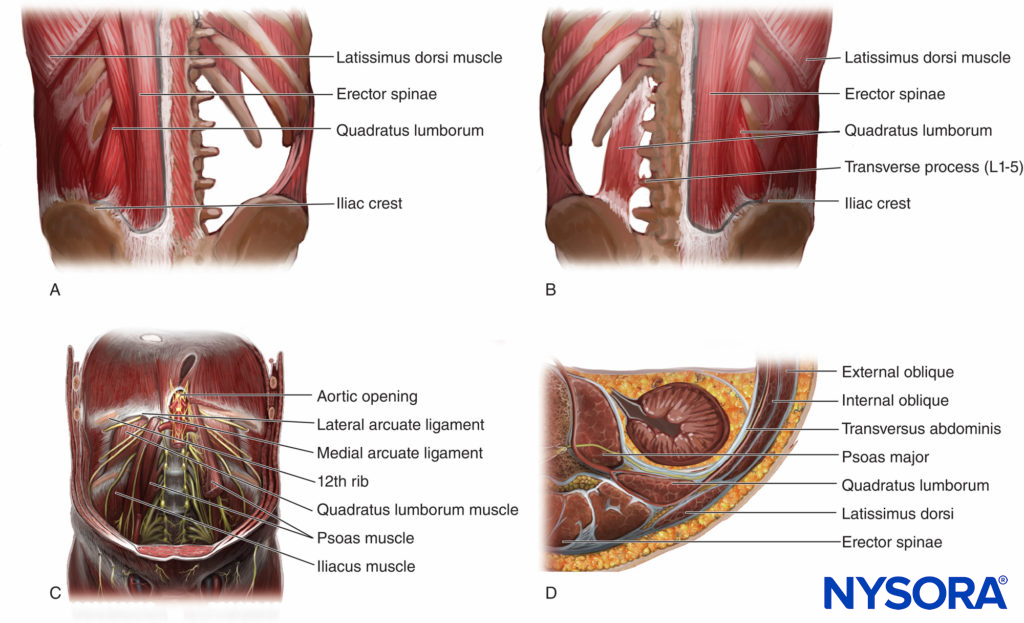
FIGURE 3. The quadratus lumborum (QL) muscle in four views: A: QL muscle from the back covered by the erector spinae and latissimus dorsi muscles. B: QL muscle from the back, with ES and LD muscles removed to show the origin and insertion of the QL muscle. C: QL muscle from the front, on the left side the psoas muscle is cut, showing the ventral rami of the spinal nerve roots pass in front of the QL. D: QL muscle cross section showing the surrounding muscles and the QL relation to the kidney.
The thoracolumbar fascia consists of anterior, middle, and posterior layers (Figure 4). The posterior layer of the TLF forms an attachment to the strong membranous aponeurosis of the latissimus dorsi. The three layers of the TLF are continuous with the fused posterior aponeurosis of the internal oblique and transversus abdominis muscles.
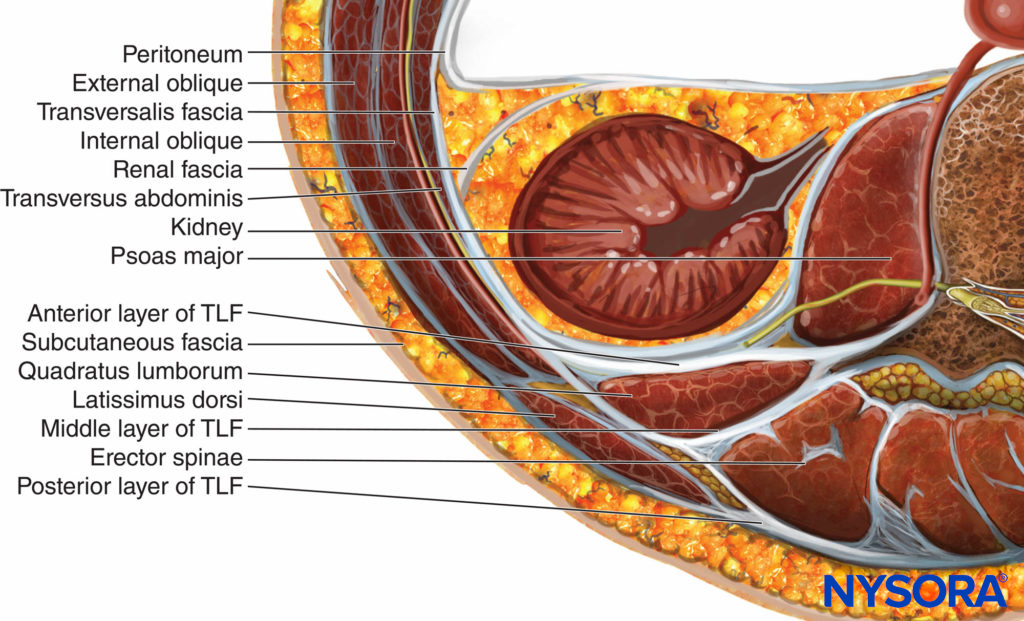
FIGURE 4. The different layers of the thoracolumbar fascia (TLF).
The posterior layer of the TLF covers the superficial side of the erector spinae. In the lumbar region, the posterior layer extends from the spinous processes medially to the lateral margin of the erector spinae, where it fuses with the middle layer of the TLF and forms the so-called lateral raphe, which is a dense connective pillar that extends from the iliac crest to the 12th rib. The deepest lamina of the posterior layer is called the paraspinal retinacular sheath (PRS), which encapsulates the erector spinae muscles. The lateral interfascial triangle (LIFT)s is made by the lateral margin of the erector spinae muscle (base), the PRS with overlying posterior and middle layers of the TLF (sides), and the lateral raphe (apex). The middle layer of the TLF separates the QL and erector spinae muscles. The anterior layer of the TLF covers the anterior aspect of the QL muscle.
The transversalis fascia (TF) invests the parietal subperitoneal areolar tissue in the abdominal cavity. The outer surface of the TF lines the deep side of the transversus abdominis, QL, and psoas major muscles. The TF communicates with the endothoracic fascia posterior to the diaphragm where the TF is thickened as the medial and lateral arcuate ligaments, with possibility of the spread of injectate from the QL and psoas major muscle compartments to the thoracic paravertebral space (Figure 5). Consequently, when the local anesthetic is injected into the fascial plane between these muscles in the lumbar region, it could spread cranially to the thoracic paravertebral space. The anterior layer of the TLF is fused with the TF. The iliohypogastric, ilioinguinal, and subcostal nerves that cross the QL muscle lie between this muscle and the TF. The four lumbar arteries on each side pass posterior to the psoas major and QL muscles, pierce the aponeurosis of the transversus abdominis muscle, and end up inside the TAP (Figure 6).
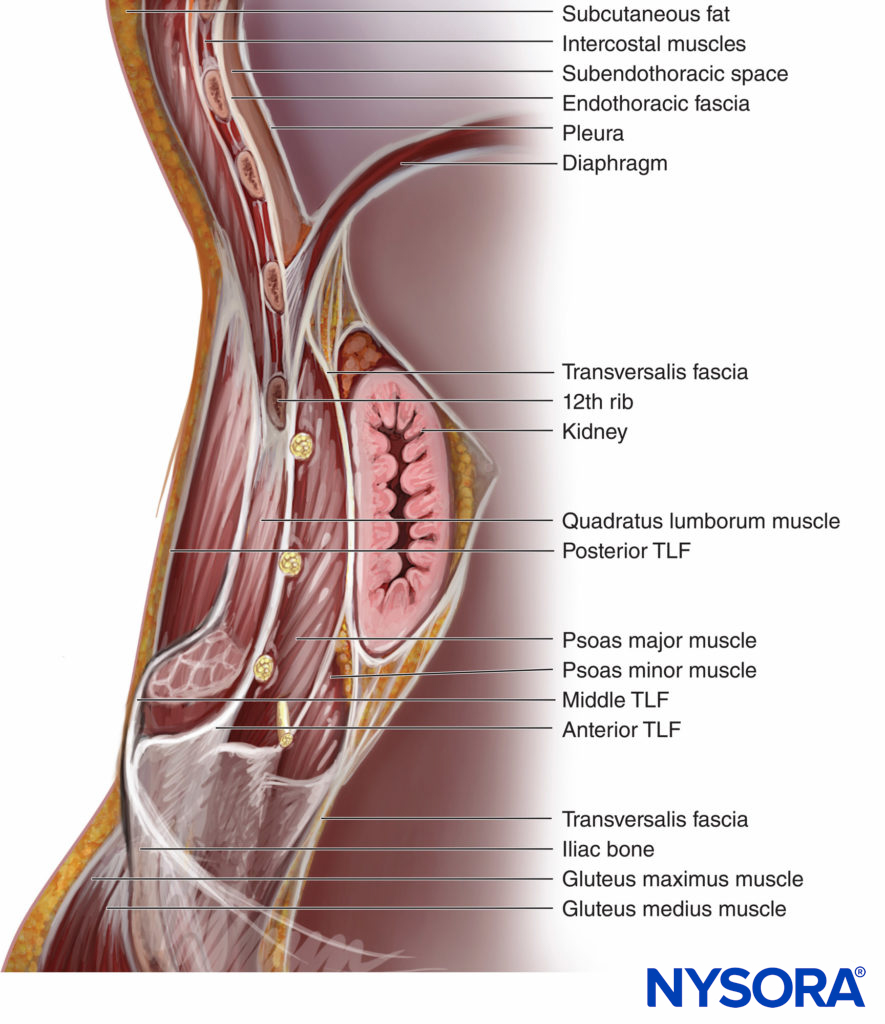
FIGURE 5. A sagittal section showing the fascial relations of the lower thoracic subendothoracic paravertebral space and the retroperitoneal space.
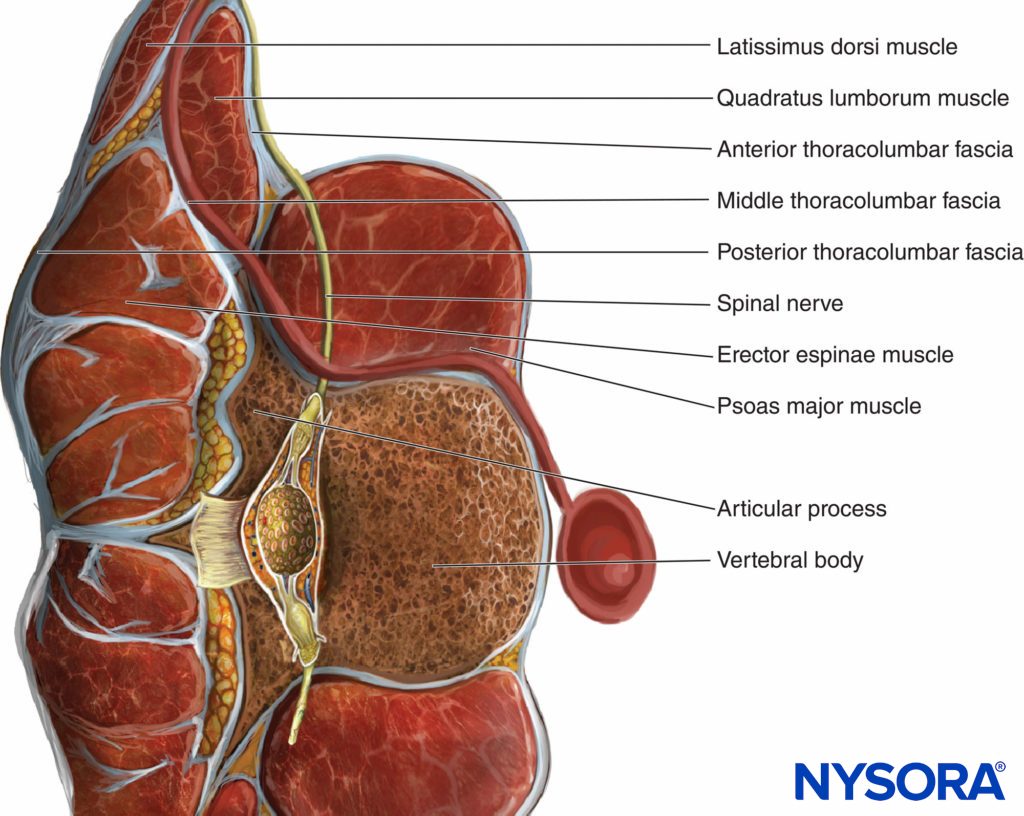
FIGURE 6. Cross section of the quadratus lumborum (QL) muscle and its relation the ventral rami of the spinal nerve roots (yellow) and the abdominal branches of the lumbar arteries (red).
The lower pole of the kidney lies anterior to the QL muscle and can reach the L4 level with deep inspiration. Therefore, this should be checked when performing QL nerve block as the kidney may be separated from the QL muscle only by perinephric fat, the posterior layer of renal fascia, the TF, and the anterior layer of the TLF. In summary, the kidney should always be visualized with QL nerve blocks to avoid kidney injury.
Learn more about Functional Regional Anesthesia Anatomy.
PATIENT POSITIONING AND EQUIPMENT SELECTION
For QL nerve blocks, the lateral decubitus position is preferred over the supine position as it provides better ergonomics and relevant sono-images of the neuraxial structures. A low-frequency (5- to 2-MHz) curved array ultrasound transducer in transverse axis is preferred to visualize the three lateral abdominal wall muscle layers and the QL muscle.
A 22-gauge, short-bevel needle is recommended for the single-injection technique, whereas an 18- to 21-gauge, 10-cm Tuohy needle with extension tubing is used for catheters. A peripheral nerve stimulator may be useful as a warning sign to prevent further needle advancement should the needle be mistakenly placed too deep and next to the lumbar plexus.
Learn more about Equipment for Peripheral Nerve Blocks
SCANNING AND NERVE BLOCK TECHNIQUES
Subcostal TAP Nerve Block
A linear transducer is placed alongside the lower margin of the rib cage as medial and cranial as possible for the subcostal TAP nerve block (Figure 7a). The rectus abdominis muscle and its posterior rectus sheath are visualized along with the transversus abdominis muscle deep to the posterior rectus sheath.
FIGURE 7. Patient and transducer position for different TAP nerve block approaches: subcostal (A), lateral (B), anterior (C), and posterior (D).
The target is the fascial plane between the posterior rectus sheath and the transversus abdominis muscle. The needle is inserted above the rectus abdominis close to the midline and advanced from medial to lateral (alternatively, lateral to medial). The endpoint of injection is the spread of local anesthetic between the posterior rectus sheath and the anterior margin of the transversus abdominis muscle. Follow the link to Truncal and Cutaneous Nerve Blocks to learn about how to perform a rectus sheath nerve block.
From the Regional Anesthesia Manual: Reverse Ultrasound Anatomy for a subcostal TAP block with needle insertion in-plane and local anesthetic spread (blue). TA, transversus abdominis; RA, rectus abdominis; IO, internal oblique; EO, external oblique muscles.
Lateral TAP Nerve Block
For the lateral TAP nerve block, a linear transducer is placed in the axial plane on the midaxillary line between the subcostal margin and the iliac crest (Figure 7b). The three layers of abdominal wall muscles are visualized: external and internal oblique as well as the transversus abdominis muscles. The target is the fascial plane between the internal oblique and the transversus abdominis muscles. The needle is inserted in the anterior axillary line, and the needle tip is advanced until it reaches the fascial plane between the internal oblique and transversus abdominis muscles approximately in the midaxillary line.
From the Regional Anesthesia Manual: Reverse Ultrasound Anatomy for a lateral TAP block with needle insertion in-plane and local anesthetic spread (blue). EO, external oblique; IO, internal oblique; transversus abdominis muscles.
Anterior TAP Nerve Block
A linear transducer is placed medial to the anterior superior iliac spine pointing toward the umbilicus with a caudad tilt for the anterior TAP nerve block (Figure 7c). The three abdominal wall muscles are visualized (see discussion for the lateral TAP nerve block). The target is the same fascial plane at the level of the deep circumflex iliac artery. The needle is inserted medial to the anterior superior iliac spine. The needle tip is advanced until it is placed between the internal oblique and transversus abdominis muscles adjacent to the deep circumflex iliac artery.
From the Regional Anesthesia Manual: Reverse Ultrasound Anatomy for an anterior TAP block with needle insertion in-plane and local anesthetic spread (blue). EO, external oblique; IO, internal oblique; transversus abdominis muscles.
Posterior TAP Nerve Block
For the posterior TAP nerve block, the linear transducer is placed in the axial plane in the midaxillary line and moved posteriorly to the most posterior limit of the TAP between the internal oblique and transversus abdominis muscles (Figure 7d). The target is the most posterior end of the TAP. The needle is inserted in the midaxillary line and advanced posteriorly until it reaches the posterior end of the TAP.
From the Regional Anesthesia Manual: Reverse Ultrasound Anatomy for a posterior TAP block with needle insertion in-plane and local anesthetic spread (blue). TA, transversus abdominis; IO, internal oblique; EO, external oblique; QL, quadratus lumborum muscles.
Transmuscular QL Nerve Block
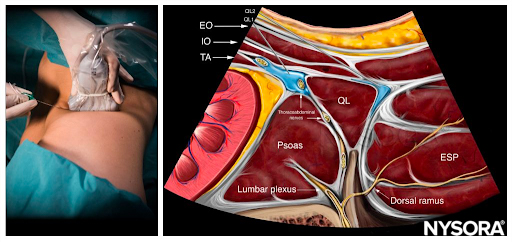
A curved array transducer for the transmuscular QL (TQL) nerve block is placed in the axial plane on the patient’s flank just cranial to the iliac crest. The “shamrock sign” is visualized: The transverse process of vertebra L4 is the stem, whereas the erector spinae posteriorly, QL laterally, and psoas major anteriorly represent the three leaves of the trefoil. The target for injection is the fascial plane between the QL and psoas major muscles (Figure 8). The needle is inserted using an in-plane technique from the posterior end of the transducer through the QL muscle (Figure 9). The injectate should ideally spread from the injection site inside the fascial plane between the QL and psoas major muscles to the thoracic paravertebral space with a goal to accomplish segmental somatic and visceral analgesia from T4 to L1. The needle approaches of the QLBs are shown in Figure 10.
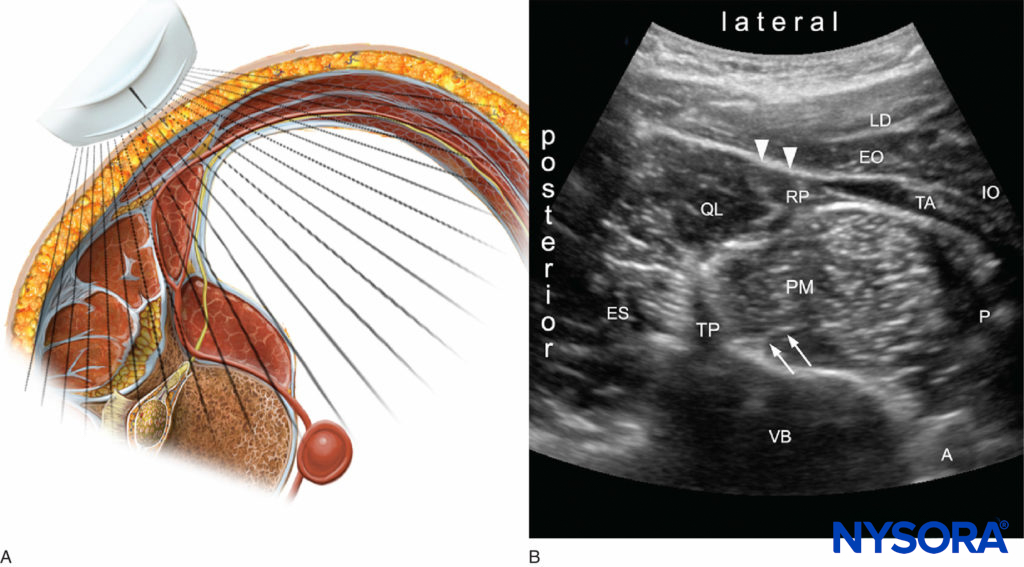
FIGURE 8. Cross section with the ultrasound probe location. B: Ultrasound image of the lateral abdominal wall. QL = quadratus lumborum; PM = psoas major; ES = erector spinae; TP = transverse process; VB = vertebral body (L4); TA = transverse abdominis; IO = internal oblique; EO = external oblique; LD = latissimus dorsi; RP = retroperitoneal space; P = peritoneal space; A = aorta; arrows = lumbar plexus; arrow heads = transversus abdominis aponeurosis.
FIGURE 9. Patient and transducer position for Transmuscular QLB.
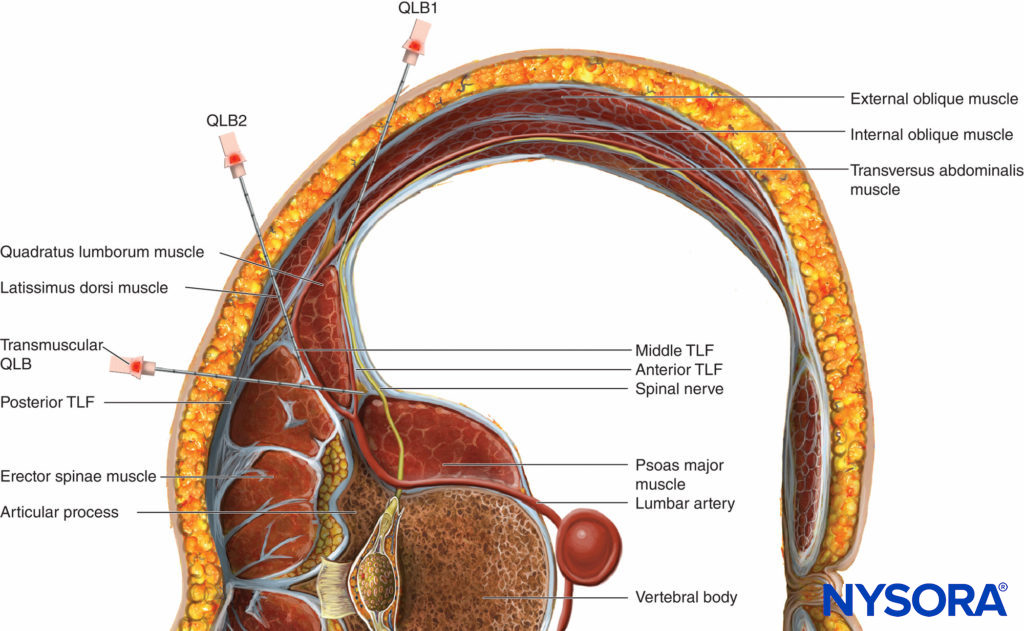
FIGURE 10. Trajectory of the needle for all three approaches of the quadratus lumborum (QL) nerve block (QLB1, QLB2, and QLB3).
From the Regional Anesthesia Manual: Reverse Ultrasound Anatomy for a transmuscular QL block with needle insertion in-plane and local anesthetic spread (blue). EO, external oblique; IO, internal oblique; TA, transversus abdominis; QL, quadratus lumborum; PMM, psoas major; ESP, erector spinae muscles.
Type 1 QL Nerve Block
For the type 1 QL (QL1) nerve block, a linear transducer is placed in the axial plane in the midaxillary line and moved posteriorly until the posterior aponeurosis of the transversus abdominis muscle becomes visible as a strong specular reflector. The target is just deep to the aponeurosis but superficial to the TF at the lateral margin of the QL muscle. This is just lateral to the pararenal fat compartment. The QL1 nerve block is identical to the fascia transversalis plane nerve block. The needle is inserted from either the anterior or the posterior end of the transducer and advanced until the needle tip just penetrates the posterior aponeurosis of the transversus abdominis muscle. Local anesthetic is injected between the aponeurosis and the TF at the lateral margin of the QL muscle. The main effect is anesthesia of the lateral cutaneous branches of the iliohypogastric, ilioinguinal, and subcostal nerves (T12–L1).
Type 2 QL Nerve Block
In the type 2 QL (QL2) nerve block, a linear transducer is placed in the axial plane in the midaxillary line and moved posteriorly as in the QL1 nerve block, until the LIFT, which encapsulates the paraspinal muscles, becomes visible between the latissimus dorsi and QL muscles.
The target is the deep layer (the PRS) of the middle layer of the TLF. The needle is inserted from the lateral end of the transducer. The needle tip is advanced until it is inside the middle layer of the TLF close to the LIFT. The local anesthetic is injected intrafascially and apparently provides analgesia equivalent to TQL nerve block but with faster onset. The mechanism of action is not well understood.
From the Regional Anesthesia Manual: Reverse Ultrasound Anatomy for a QL1 and QL2 block with needle insertion in-plane and local anesthetic spread (blue). EO, external oblique; IO, internal oblique; TA, transversus abdominis; QL, quadratus lumborum; ESP, erector spinae muscles.
DOSE AND VOLUME OF LOCAL ANESTHETIC
The TAP nerve blocks as well as the TQL nerve block and QLB1 are “tissue plane” nerve blocks and thus require large volumes of local anesthetic to obtain reliable block. For each of the TAP nerve blocks, a minimum volume of 15 mL is recommended. The local anesthetic dose needs to be considered for the size of the patient to ensure that a maximum safe dose is not exceeded, especially with dual bilateral TAP nerve blocks. The QL region is relatively vascular as the lumbar arteries lie posterior to the muscle. Absorption of the local anesthetic into the circulation depends primarily on the vascularity of the site of deposition. As the QL muscle is well vascularized and a large volume of local anesthetic is needed, the dose should be calculated accurately to prevent high peak plasma concentrations of local anesthetics in this type of nerve block.
For additional information follow the link to Clinical Pharmacology of Local Anesthetics
INDICATIONS
Most of the indications for QL nerve blocks are based on case reports and clinical anecdotal experience. There are no studies comparing the safety and efficacy of the three types of QL nerve block. Table 1 compares and summarizes the three types of QL nerve blocks.
TABLE 1. Main features of QL nerve blocks.
| QLB1 | QLB2 | TQLB | |
|---|---|---|---|
| Clinical indications | Abdominal surgery below the umbilicus. | Abdominal surgery either above or below the umbilicus (any type of operation that requires intra-abdominal visceral pain coverage and abdominal wall incisions as high as T6) | Abdominal surgery either above or below the umbilicus (any type of operation that requires intra-abdominal visceral pain coverage and abdominal wall incisions as high as T6) |
| Dermatomes covered | L1 | T4 to T12-L1; blocks the anterior and the lateral cutaneous branches of the nerves | T4 to T12-L1; blocks the anterior and the lateral cutaneous branches of the nerves |
| Lower extremity weakness | Not reported | Not reported | Potential |
| Spread to lumbar plexus | Not reported | Not reported | Potential |
| Needle entry and approach | Lateral abdomen near the posterior axillary line, below the costal margin and above the iliac crest and inserting the needle inplane with the curved array probe oriented axially. | Lateral abdomen near the posterior axillary line, below the costal margin and above the iliac crest and inserting the needle inplane with the curved array probe oriented axially. | Lateral abdomen near the posterior axillary line, below the costal margin and above the iliac crest and inserting the needle inplane with the curved array probe oriented axially. |
| Potential complications | Complications are related to the lack of anatomical understanding and needle expertise. It is possible to puncture intra-abdominal structures such as the kidney, liver, and spleen. | Complications are related to the lack of anatomical understanding and needle expertise. It is possible to puncture intra-abdominal structures such as the kidney, liver, and spleen. | Complications are related to the lack of anatomical understanding and needle expertise. It is possible to puncture intra-abdominal structures such as the kidney, liver, and spleen. |
| Injection site | Potential space medial to the abdominal wall muscles and lateral to QL muscle, anterolateral border of the QL muscle, at the junction with the transversalis fascia, outside the anterior layer of the TLF and fascia transversalis | Posterior to the QL muscle, outside the middle layer of the TLF | Anterior to the QL muscle, between the QL and the psoas major muscles, outside the anterior layer of the TLF and fascia transversalis, close to the intervertebral foramen |
| Level of difficulty | Intermediate | Intermediate | Advanced |
The various QL nerve blocks share the same indications as of the TAP nerve block. Some examples are as follows:
- Large-bowel resection, open/laparoscopic appendectomy, and cholecystectomy
- Cesarean section, total abdominal hysterectomy
- Open prostatectomy, renal transplant surgery, nephrectomy, abdominoplasty, iliac crest bone graft
- Ileostomy
- Exploratory laparotomy, bilateral nerve blocks for midline incisions
NYSORA Tips
• Close to the transverse process, the QL muscle appears thin as it is visualized anterior-posterior; visualized from the flank, the muscle looks much broader.
• Use color Doppler before insertion of the needle to detect the lumbar arteries on the posterior aspect of the QL muscle or any other large vessels.
• The QL is identified medial to the transversus abdominis muscle. The latissimus dorsi and erector spinae muscles are superficial and more hyperechoic.
SUMMARY
The various TAP nerve blocks can provide somatic analgesia for abdominal wall surgery. QL nerve blocks can provide somatic as well as visceral analgesia of both the abdominal wall and the lower segments of the thoracic wall and therefore could be a useful analgesic modality for selected abdominal surgeries. QL nerve blocks may provide visceral analgesia due to their paravertebral and possibly epidural spread. The information in this chapter is based on the current knowledge, with an understanding that more specific recommendations are pending a stronger evidence base.
Clinical updates
Joshi et al. (Anesthesiology, 2026) publish updated American Society of Anesthesiologists practice guidelines strongly recommending ultrasound-guided fascial plane blocks to reduce pain and opioid consumption in the first 24 hours after open cardiothoracic, abdominal, pelvic surgery, and mastectomy in adults, with moderate-quality evidence showing clinically meaningful opioid reductions (≈35–60 oral morphine equivalents). For minimally invasive abdominal surgery, fascial plane blocks are also strongly recommended for opioid sparing, while recommendations for minimally invasive cardiothoracic surgery and open hernia repair remain conditional due to low-quality evidence. In children, fascial plane blocks are strongly recommended after open cardiac or thoracic surgery; however, overall conclusions are limited by heterogeneity, lack of blinding, and small single-center trials, underscoring the need for standardized outcomes and higher-quality studies.
- Read more about the study HERE.
Turunc et al. (Regional Anesthesia & Pain Medicine, 2025) report that bilateral anterior subcostal quadratus lumborum block (QLB) significantly reduces opioid consumption after laparoscopic colorectal surgery, lowering 24-hour IV morphine equivalents by ~9 mg and consistently improving pain scores at rest and with movement. The block also prolonged the time to first PCA request, markedly reduced rescue analgesic and antiemetic use, and was associated with earlier mobilization and a one-day shorter hospital stay, without observed block-related complications. These findings suggest anterior subcostal QLB may provide clinically meaningful opioid-sparing and recovery benefits within ERAS pathways, though confirmation in larger multicenter trials is needed.
Keller et al. (Regional Anesthesia & Pain Medicine, 2025) report that a single-shot bilateral oblique subcostal TAP (OSTAP) block for open sublay mesh hernia repair provides early analgesic benefit in the PACU with slightly lower immediate morphine use, but fails to reduce opioid consumption by postoperative day 2. In fact, patients receiving ropivacaine required significantly more opioids and reported higher peak pain scores later, consistent with rebound pain after block resolution, while adverse events and length of stay were similar. These findings suggest that OSTAP blocks alone are insufficient for sustained analgesia in this setting and should be combined with multimodal strategies, adjuvants, or catheter-based techniques, as appropriate.
- Read more about the study HERE.
Rozier et al. (Regional Anesthesia & Pain Medicine, 2025) report in a two-center randomized placebo-controlled trial that adding an anterior quadratus lumborum block (20 mL 0.2% ropivacaine) to a comprehensive multimodal analgesia regimen for primary total hip arthroplasty does not reduce 24-hour opioid consumption compared with sham. Pain scores, patient experience, early mobilization metrics, quadriceps strength, and 3-month functional outcomes were also not different between groups, with no block-related complications observed. These data suggest routine anterior QLB provides no additional benefit when effective NSAID-based multimodal analgesia is already in place for THA.
- Read more about the study HERE.
Hay et al. (Regional Anesthesia & Pain Medicine, 2026) report in a randomized controlled trial of 101 patients undergoing primary total hip arthroplasty that lateral quadratus lumborum block (QLB) results in significantly lower cumulative opioid consumption from 36–72 hours postoperatively compared with PENG plus lateral femoral cutaneous nerve block, with a mean difference of ~33 mg IV morphine equivalents at 72 hours. Patients receiving lateral QLB also had lower pain scores with movement, while pain at rest, time to ambulation, same-day discharge rates, length of stay, motor recovery, and patient-reported functional outcomes were similar between groups. These findings suggest lateral QLB may better mitigate late postoperative pain and opioid use after THA, potentially reducing rebound pain seen with more focal motor-sparing blocks.
- Read more about the study HERE.
Giral et al. (Regional Anesthesia & Pain Medicine, 2024) report in a prospective randomized trial of 104 parturients that bilateral posterior quadratus lumborum block (PQLB) provides similar 24-hour opioid consumption to intrathecal morphine after scheduled cesarean section, with no differences in pain at rest. PQLB was associated with less pruritus, longer time to first morphine request, lower dynamic pain at 6 hours, and better early recovery quality. These findings suggest PQLB is a reasonable alternative to intrathecal morphine in opioid-intolerant patients, offering comparable analgesia with fewer opioid-related side effects.
- Read more about the study HERE.
Park et al. (Reg Anesth Pain Med, 2026) conducted a randomized non-inferiority trial showing that bilateral TAP block combined with intrathecal fentanyl did not achieve non-inferior analgesia compared with intrathecal morphine after cesarean delivery, with higher 24-hour pain scores and significantly greater postoperative opioid consumption (585 vs 140 µg fentanyl). However, intrathecal morphine caused substantially more pruritus (60% vs 10%), indicating that while morphine remains superior for analgesia, TAP block with intrathecal fentanyl may be a reasonable alternative when minimizing opioid-related side effects is prioritized.
- Read more about this HERE.