Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About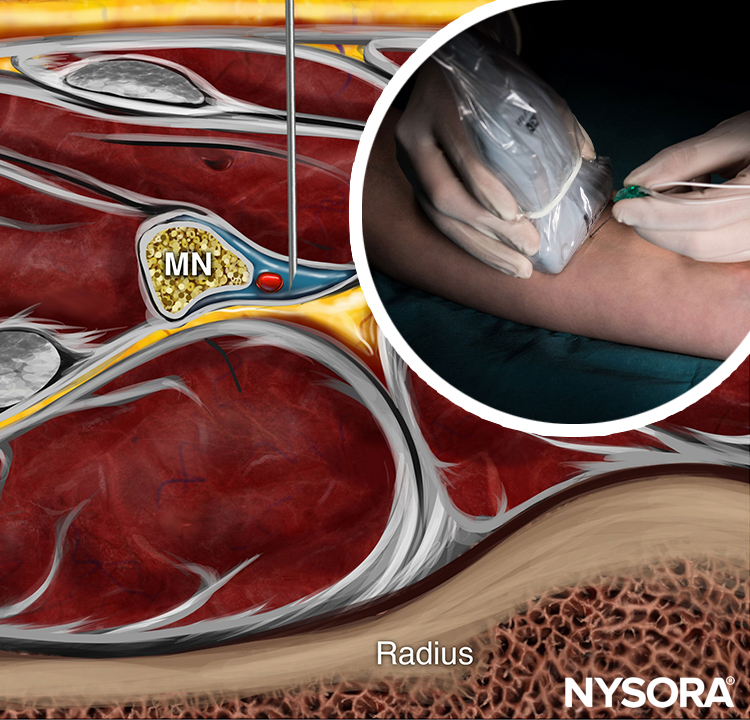
FACTS
- Indications: Hand and finger surgery
- Transducer position: Transverse at wrist crease or distal third of the forearm (Figure 1)
- Goal: Local anesthetic injection next to the median and ulnar nerves and the sensory branch of the radial nerve
- Local anesthetic: 10–15 mL (total volume)

FIGURE 1. Ultrasound-guided wrist nerve block. Transducer and needle positions for (A) median nerve block; (B) ulnar nerve block; (C) radial nerve block.
GENERAL CONSIDERATIONS
The wrist nerve block is an effective method to provide anesthesia of the hand and fingers without the arm immobility that occurs with more proximal brachial plexus nerve blocks. Traditional wrist nerve block technique involves advancing needles using surface landmarks toward the three nerves that supply the hand: the median, ulnar, and radial nerves. Since the nerves are located relatively close to the surface, this is a technically easy nerve block to perform, but knowledge of the anatomy of the soft tissues of the wrist is essential for successful block with minimum patient discomfort. In addition to providing anesthesia and analgesia, wrist nerve blocks using botulinum toxin to treat hyperhidrosis have been described.
ULTRASOUND ANATOMY
Three individual nerves are involved in a wrist nerve block: the median, ulnar, and radial nerves.
The Median Nerve
The median nerve crosses the elbow medial to the brachial artery and courses toward the wrist deep to the flexor digitorum superficialis in the center of the forearm. As the muscles taper toward tendons near the wrist, the nerve assumes an increasingly superficial position until it is located beneath the flexor retinaculum in the carpal tunnel with the tendons of the flexor digitorum profundus, flexor digitorum superficialis, and flexor pollicis longus. A linear transducer placed transversely at the level of the wrist crease will reveal a cluster of oval hyperechoic structures, one of which is the median nerve. At this location, it is easy to confuse the tendons for the nerve and vice versa; for this reason, it is recommended to slide the transducer 5–10 cm proximally the volar side of the forearm, to confirm the location of the nerve. The tendons will have disappeared on the image, leaving just muscle and the solitary median nerve (Figures 2 and 3), which then can be carefully traced back to the wrist, if desired. In many instances, however, it is much simpler to perform a median nerve block at the midforearm, where the nerve is easier to recognize.
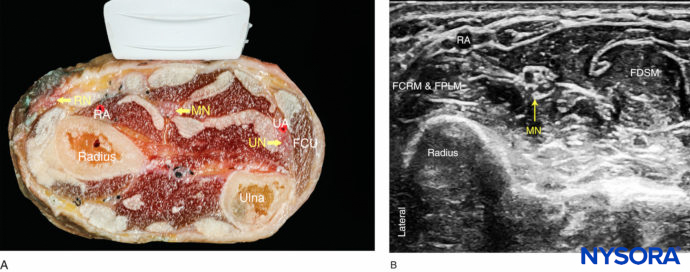
FIGURE 2. (A) Cross-sectional anatomy of the distal forearm. (B) Sonoanatomy of the median nerve (MN) at the forearm. RA, radial artery; FCRM, flexor carpi radialis muscle; FPLM, flexor pollicis longus muscle; FDSM, flexor digitorum superficialis muscle.

FIGURE 3. Cross-sectional ultrasound image of the median nerve (MN) at the wrist. Needle path to reach the MN at the wrist and spread of local anesthetic to nerve block the MN.
The Ulnar Nerve
The ulnar nerve is located medially (ulnar side) to the ulnar artery from the level of the mid-forearm to the wrist; this provides a useful landmark. A linear transducer placed at the level of the wrist crease will show the hyperechoic anterior surface of the ulna with shadowing behind; just lateral to the bone and very superficial will be the triangular or oval hyperechoic ulnar nerve, with the pulsating ulnar artery immediately next to it (Figures 4 and 5). At this location, the tendon of the flexor carpis ulnaris muscle can be seen superficial to the ulnar nerve. Scanning proximally, these two structures can be easily differentiated. Sliding the transducer up and down the forearm helps verify that the structure is the ulnar nerve by following the course of the ulnar artery and looking for the nerve on its ulnar side.
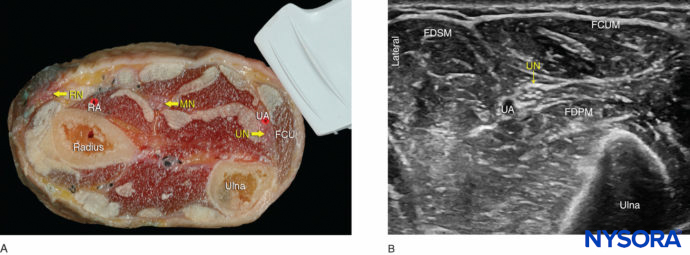
FIGURE 4. (A) Cross-sectional anatomy of the distal forearm. (B) Sonoanatomy of the ulnar nerve (UN) at the forearm. UA, ulnar artery; FCUM, Flexor carpi ulnaris. FDPM, flexor digitorum profundus muscle; FDSM, flexor digitorum superficialis muscle.

FIGURE 5. Sonoanatomy of the ulnar nerve (UN) at the wrist: needle path to reach the UN at the wrist and approximate spread of local anesthetic (blue-shaded area) to anesthetize the UN. UA, ulnar artery.
The Radial Nerve
The superficial branch of the radial nerve divides into terminal branches at the level of the wrist; for this reason, ultrasonography is not very useful for nerve block placement guidance at the level of the wrist. A subcutaneous field nerve block around the area of the styloid process of the radius remains an easy method to perform an effective radial nerve block at the level of the wrist. However, ultrasonography can be used at the level of the elbow or in the mid-forearm. At this level, the nerve is identified as a thin hyperechoic structure lateral to the radial artery and superficial to the radius. The nerve exits the antebrachial fascia between the tendons of the brachioradialis and the extensor carpi radialis muscles (Figures 6 and 7).
 Cross-sectional anatomy of the distal forearm. (B) Sonoanatomy of the radial nerve (RN) at the forearm. RA, radial artery.")
FIGURE 6 (A) Cross-sectional anatomy of the distal forearm. (B) Sonoanatomy of the radial nerve (RN) at the forearm. RA, radial artery.
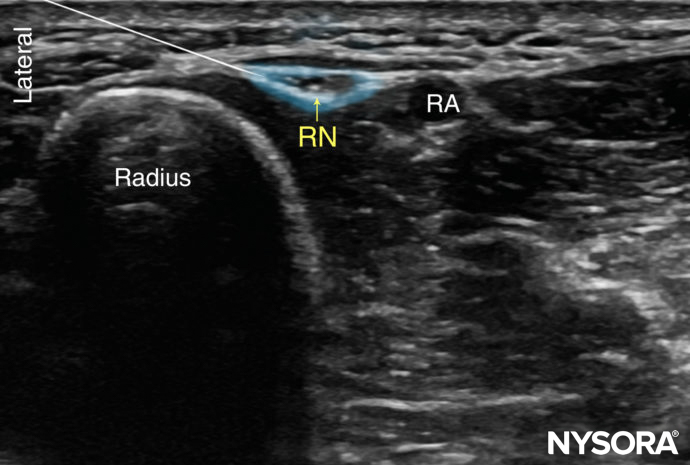
FIGURE 7. Sonoanatomy of the radial nerve (RN) at the level of the wrist. The superficial branch of the RN at the wrist is shown lateral to the radial artery (RA), and the approximate needle path to reach the branch of the radial nerve is shown with an approximate spread of local anesthetic (blue-shaded area) to anesthetize it.
DISTRIBUTION OF ANESTHESIA
A wrist nerve block results in anesthesia of the entire hand, except the territory of the deep branch of the radial nerve. For a more comprehensive review of the distribution of each terminal nerve, see Functional Regional Anesthesia Anatomy.
EQUIPMENT
The equipment needed for a wrist nerve block includes the following:
• Ultrasound machine with linear transducer (8–14 MHz), sterile sleeve, and gel
• Standard nerve block tray
• 5 mL syringes containing local anesthetic
• A 2-3 mm 22- to 25-gauge needle with low-volume extension tubing
• Sterile gloves
Learn more about Equipment for Regional Anesthesia.
LANDMARKS AND PATIENT POSITIONING
The wrist nerve block is most easily performed with the patient in the supine position to allow for the volar surface of the wrist to be exposed (Figure 1). It is useful to remove splints and/or bandages on the hand to facilitate placement of the transducer and sterile preparation of the skin surface.
GOAL
The goal of this nerve block is to place the needle tip immediately adjacent to each of the nerves to deposit local anesthetic until its spread around the nerve is documented with ultrasound visualization.
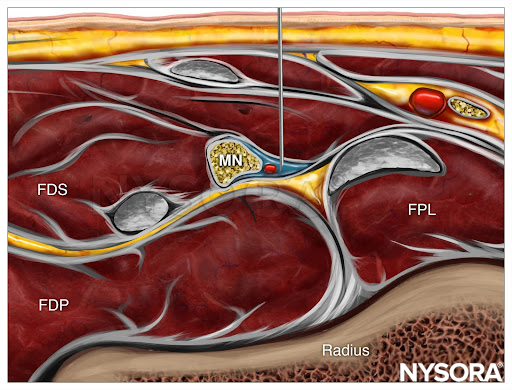
From the Regional Anesthesia Manual: Reverse Ultrasound Anatomy for a median nerve (MN) block at the level of the elbow with needle insertion out-of-plane and local anesthetic spread (blue). FPL, flexor pollicis longus; FDS, flexor digitorum superficialis; FDP, flexor digitorum profundus muscles.
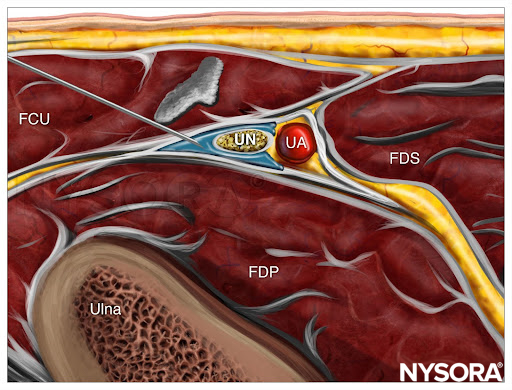
From the Regional Anesthesia Manual: Reverse Ultrasound Anatomy for an ulnar nerve (UN) block at the level of the elbow with needle insertion in-plane and local anesthetic spread (blue). UA, ulnar artery; FCU, flexor carpi ulnaris; FDP, flexor digitorum profundus; FDS, flexor digitorum superficialis muscles.
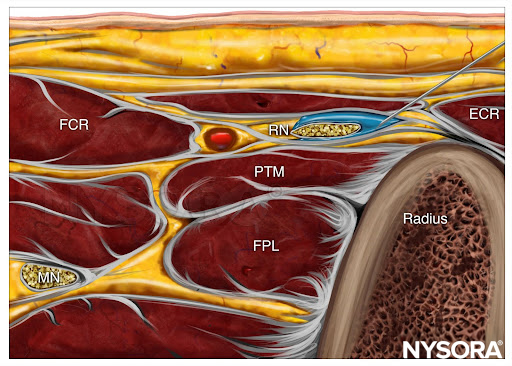
From the Regional Anesthesia Manual: Reverse Ultrasound Anatomy for a radial nerve (RN) block at the level of the elbow with needle insertion in-plane and local anesthetic spread (blue). FCR, flexor carpi radialis; MN, median nerve; FPL, flexor pollicis longus; PTM, pronator teres muscle; ECR, extensor carpi radialis.
TECHNIQUE
With the arm in the volar side up position, the skin is disinfected. The wrist is a “tightly packed” area that is bounded on three sides by bones. For this reason, a US-guided “wrist” nerve block is often performed 5–10 cm proximally to the wrist crease, where there is more room to maneuver. This location also ensures the block of the palmar branches of the median and ulnar nerves, which take off few centimeters proximally to the wrist crease. For each of the nerve blocks, the needle may be inserted either in-plane or out-of-plane. Ergonomics often dictates which is most effective. Care must be taken when performing the ulnar and radial nerve blocks since these nerves are intimately associated with arteries. Inadvertent arterial puncture can lead to hematoma. A successful nerve block is predicted by the spread of local anesthetic immediately adjacent to the nerve. Multiple injections to achieve circumferential spread are usually not necessary because these nerves are small and the local anesthetic diffuses quickly into the neural tissue due to the lack of thick epineural tissues. Assuming deposition immediately adjacent to the nerve, 3–4 mL/nerve of local anesthetic is sufficient to ensure an effective nerve block.
Clinical updates
Diéguez-García et al. (Regional Anesthesia & Pain Medicine, 2020) report in a double-blind randomized trial of 124 patients undergoing carpal tunnel surgery that circumferential local anesthetic spread around the median and ulnar nerves at the antecubital fossa produced a faster onset of complete sensory block, with significantly higher complete block rates at 5 minutes compared with non-circumferential spread. By 15–30 minutes, sensory block success was similar between techniques, although circumferential spread yielded a more complete motor block at later time points without increasing nerve swelling or neurologic complications. These data suggest that circumferential spread is mainly advantageous when a rapid, dense block onset is required, rather than for overall block success.