Thomas B. Clark, Ana M. Lopez, Daquan Xu, and Catherine Vandepitte
FACTS
- Indications: Postoperative analgesia for hip surgery, meralgia paresthetica, and muscle biopsy of the proximal lateral thigh
- Transducer position: Transverse, inferior to the anterior superior iliac spine; the lateral edge of the sartorius muscle should be visualized with ultrasound
- Goal: Local anesthetic spread around LFCN between the tensor fasciae latae and sartorius muscles
- Local anesthetic: 5 mL (adults)
GENERAL CONSIDERATIONS
The lateral femoral cutaneous nerve (LFCN) divides into several branches innervating the lateral and anterior aspects of the thigh. Of note, in 45% of patients, innervation of the LFCN extends even to the anterior thigh. The variable anatomy of the lateral femoral cutaneous nerve makes it challenging to perform an effective landmark-based block. US guidance, however, allows for more accurate needle insertion into the appropriate fascial plane through which the LFCN passes.
ULTRASOUND ANATOMY
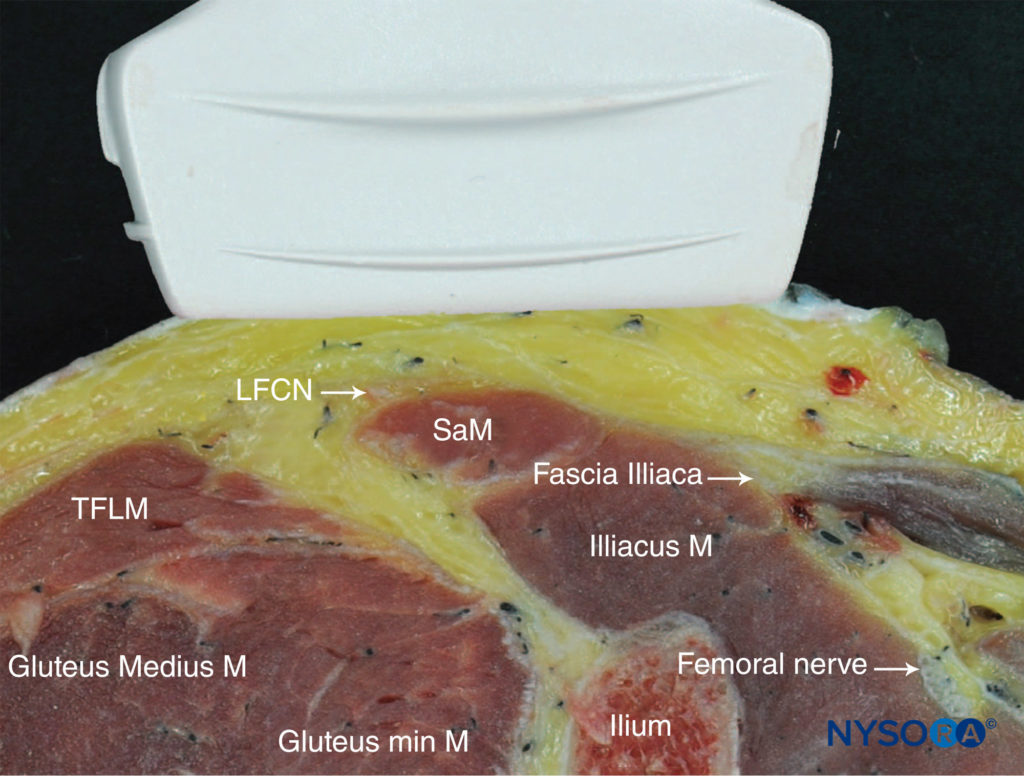
The LFCN typically is visualized between the tensor fasciae latae muscle (TFLM) and the sartorius muscle (SaM), 1–2 cm medial and inferior to the anterior superior iliac spine (ASIS) and 0.5–1.0 cm deep to the skin surface (Figure 1). Ultrasound (US) imaging of the LFCN yields an oval hypoechoic small structure with a hyperechoic rim that can be easily seen in the hypoechoic background. The LFCN can be traced proximally, as it runs from the lateral to the medial edge of the superficial fascia of the SaM. The lateral edge of the SaM is a useful landmark, and as such, it can be relied on throughout the procedure. The posterior branch of the LFCN may sometimes be seen across the anterior margin of the TFLM.
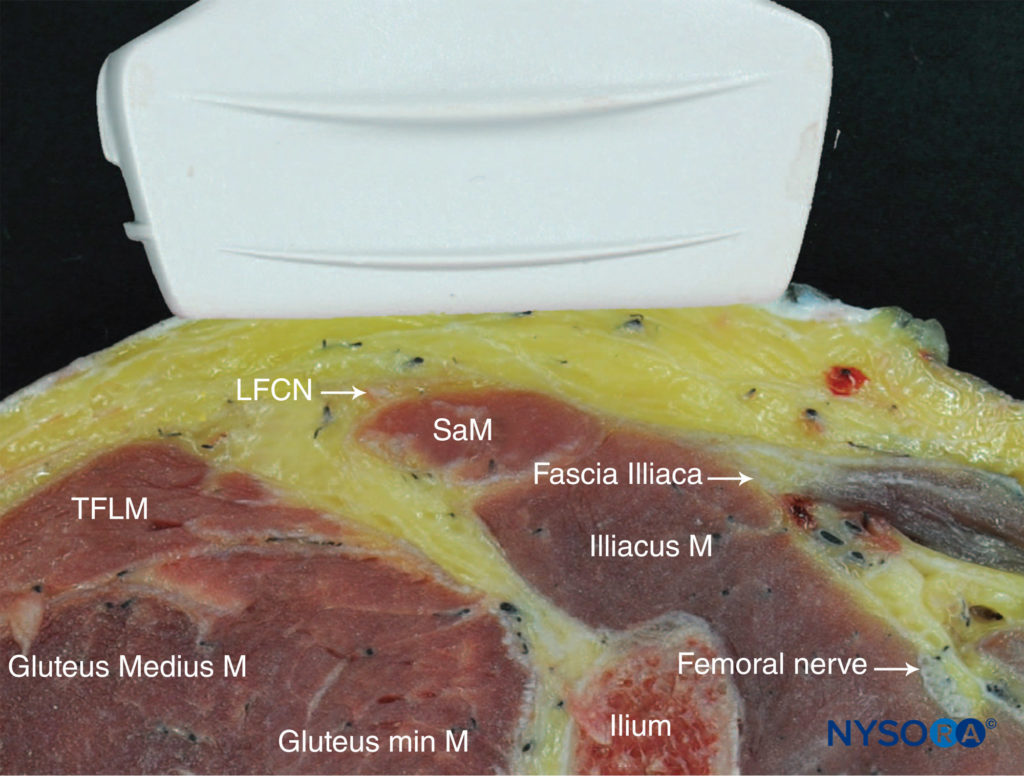
FIGURE 1. Cross-sectional anatomy of the lateral femoral cutaneous nerve (LFCN). Shown are the LFCN, sartorius muscle (SaM), and tensor fasciae latae muscle (TFLM). (Reproduced with permission from Hadzic A: Hadzic’s Peripheral Nerve Blocks and Anatomy for Ultrasound-Guided Regional Anesthesia, 2nd ed. New York: McGraw-Hill, 2011.)
DISTRIBUTION OF ANESTHESIA
Block of the LFCN provides anesthesia or analgesia in the anterolateral thigh. There is a large variation in the area of sensory coverage among individuals because of the highly variable course of the LFCN and its branches (Figure 2).

FIGURE 2. Expected distribution of lateral femorocutaneous nerve sensory block.
EQUIPMENT
The equipment recommended for an LFCN block is as follows:
- Ultrasound machine with a linear transducer (18-6 MHz), sterile sleeve, and gel
- Standard nerve block tray
- Syringe(s) with 10 mL of local anesthetic
- 3–5 cm, 22- to 24-gauge needle
- Sterile gloves
Learn more about Equipment for Regional Anesthesia.
LANDMARKS AND PATIENT POSITIONING
Block of the LFCN is performed with the patient in the supine or lateral position. Palpation of the anterior superior spine provides the initial landmark for transducer placement; the transducer is first positioned at 2 cm inferior and medial to the ASIS and adjusted accordingly. Typically, the nerve is identified slightly more distally in its course. Additional confirmation of the correct identification of the LFCN may be made by eliciting a tingling sensation on the lateral side of the thigh using a nerve stimulator.
GOAL
The goal is to inject local anesthetic in the plane between the TFLM and the SaM, typically 1–2 cm medial and inferior to the ASIS.
TECHNIQUE
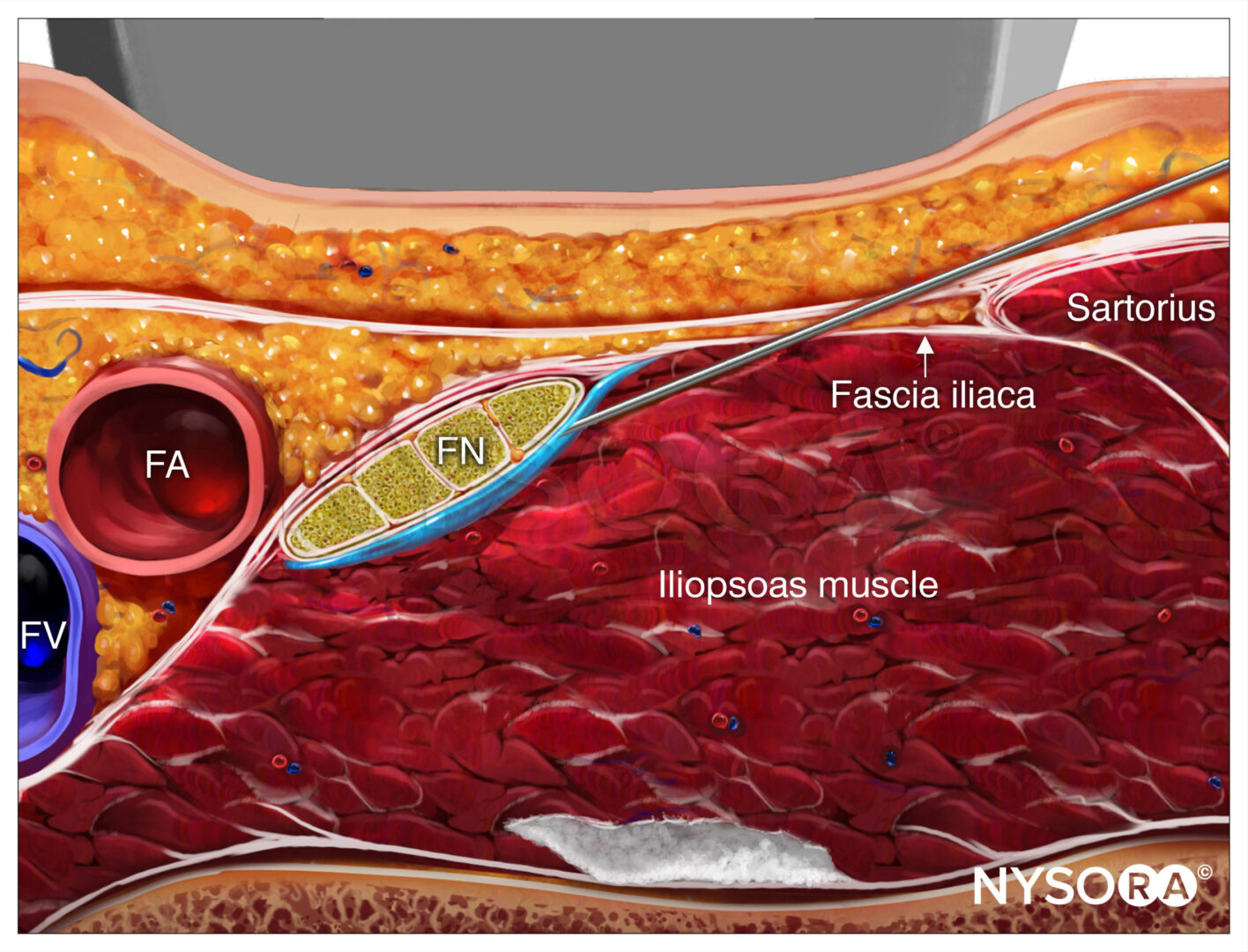
With the patient supine, the skin is disinfected and the transducer placed immediately inferior to the ASIS, parallel to the inguinal ligament (Figure 3). The TFLM and SaM are then identified. The nerve should appear as a small hypoechoic oval structure with a hyperochoic rim between the TFLM and SaM in a short-axis view or superficial to the SaM (Figure 4a).
FIGURE 3. Transducer position to accomplish a lateral femoral cutaneous nerve (LFCN) block.
 Ultrasound anatomy of the lateral femoral cutaneous nerve (LCFN). (B) Simulated needle path and local anesthetic spread (blue-shaded area) to anesthetize the LFCN.")
FIGURE 4. (A) Ultrasound anatomy of the lateral femoral cutaneous nerve (LCFN). (B) Simulated needle path and local anesthetic spread (blue-shaded area) to anesthetize the LFCN.
The needle is inserted in plane in a lateral-to-medial orientation, through the subcutaneous tissue. A fascial “pop” or “click” may be felt as the needle tip enters the plane between the TFLM and SaM. A volume of 1–2 mL of local anesthetic is injected to verify the needle tip position. The correct position is achieved by visualizing the spread of local anesthetic in the described plane between the TFLM and SaM or around the LFCN superficial to the SaM (Figure 4b).
TIPS
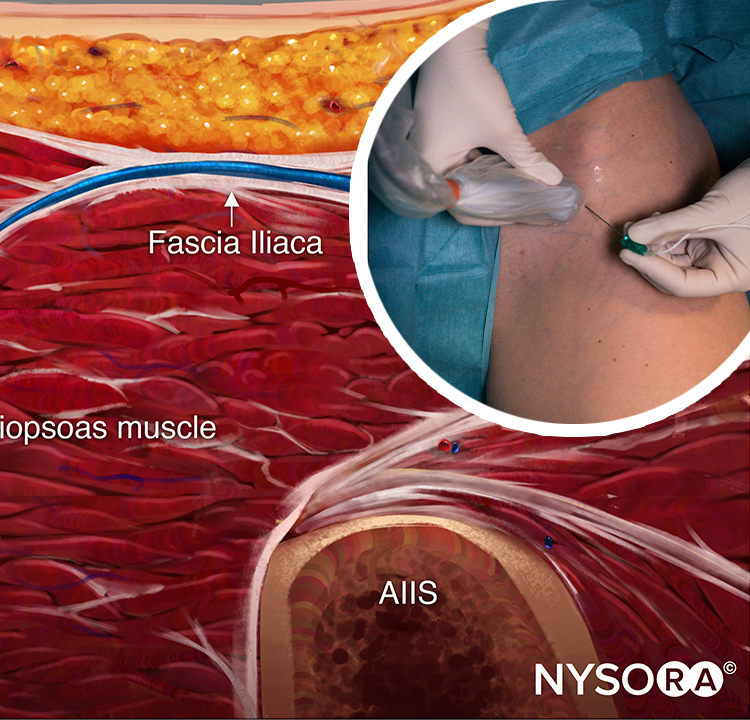
- A “subinguinal” technique has also been described, in which the US probe straddles the ASIS and the anterior inferior iliac spine (AIIS). Local anesthetic is injected under the inguinal ligament, 1–2 cm medial to the ASIS, without necessarily attempting to visualize the nerve.
- In an adult patient, 5 mL of local anesthetic is usually sufficient. In children, a volume of 0.15 mL/kg per side is adequate for effective analgesia.
For a more comprehensive review continue reading Ultrasound-Guided Fascia Iliaca Block
REFERENCES
- Corujo A, Franco CD, Williams JM: The sensory territory of the lateral cutaneous nerve of the thigh as determined by anatomic dissections and ultrasound-guided blocks. Reg Anesth Pain Med 2012;37:561–564.
- Moritz T, Prosch H, Berzaczy D, et al: Common anatomical variation in patients with idiopathic meralgia paresthetica: a high resolution ultrasound case-control study. Pain Physician 2013;16:E287–293.
- Hara K, Sakura S, Shido A: Ultrasound-guided lateral femoral cutaneous nerve block: comparison of two techniques. Anaesth Intensive Care 2011;39:69–72.
- Bodner G, Bernathova M, Galiano K, Putz D, Martinoli C, Felfernig M: Ultrasound of the lateral femoral cutaneous nerve: normal findings in a cadaver and in volunteers. Reg Anesth Pain Med 2009;34:265–268.
- Carai A, Fenu G, Sechi E, Crotti FM, Montella A: Anatomical variability of the lateral femoral cutaneous nerve: findings from a surgical series. Clin Anat 2009;22:365–370.
- Damarey B, Demondion X, Boutry N, Kim HJ, Wavreille G, Cotten A: Sonographic assessment of the lateral femoral cutaneous nerve. J Clin Ultrasound 2009;37:89–95.
- Hara K, Sakura S, Shido A: Ultrasound-guided lateral femoral cutaneous nerve block: comparison of two techiques. Anaesth Intensive Care 2011;39: 69–72.
- Hebbard P, Ivanusic J, Sha S: Ultrasound-guided supra-inguinal fascia iliaca block: a cadaveric evaluation of a novel approach. Anaesthesia 2011;66:300–305.
- Hurdle MF, Weingarten TN, Crisostomo RA, Psimos C, Smith J: Ultrasoundguided block of the lateral femoral cutaneous nerve: technical description and review of 10 cases. Arch Phys Med Rehabil 2007;88:1362–1364.
- Ng I, Vaghadia H, Choi PT, Helmy N: Ultrasound imaging accurately identifies the lateral femoral cutaneous nerve. Anesth Analg 2008;107:1070–1074.
- Ropars M, Morandi X, Huten D, Thomazeau H, Berton E, Darnault P: Anatomical study of the lateral femoral cutaneous nerve with special reference to minimally invasive anterior approach for total hip replacement. Surg Radiol Anat 2009;31:199–204.
- Sürücü HS, Tanyeli E, Sargon MF, Karahan ST: An anatomic study of the lateral femoral cutaneous nerve. Surg Radiol Anat 1997;19:307–310.
- Tumber PS, Bhatia A, Chan VW: Ultrasound-guided lateral femoral cutaneous nerve block for meralgia paresthetica. Anesth Analg 2008;106:1021–1022.