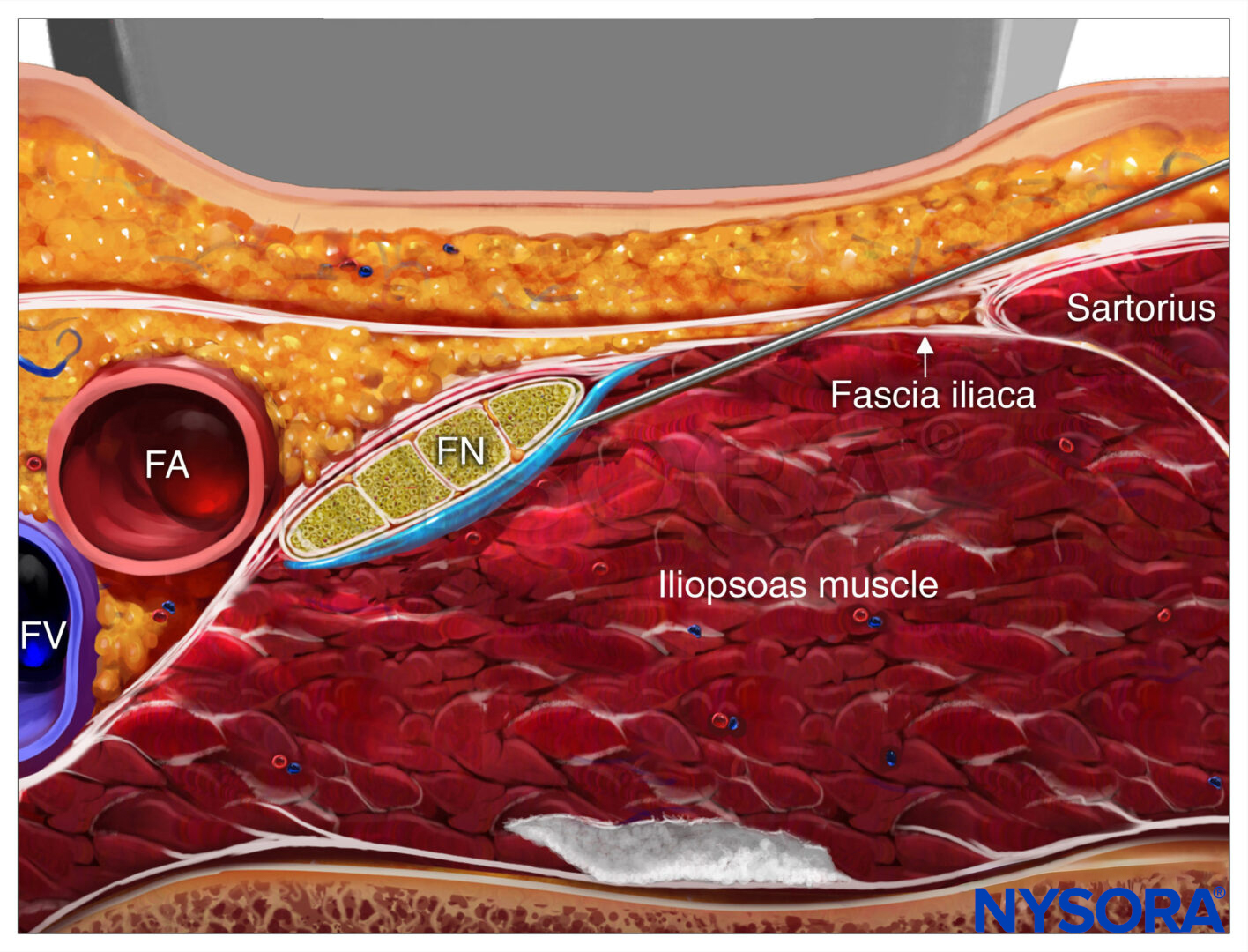
Figure 1: (A) Transducer position and needle insertion to accomplish a transverse abdominal plane nerve block. (B) Transducer position and needle insertion to accomplish iliohypogastric and ilioinguinal nerve blocks. (C) Transducer position and needle insertion to accomplish rectus sheath nerve block. (D) Transducer position and needle insertion to accomplish a lateral femoral cutaneous nerve (LFCN) block. Essentials A – TRANSVERSUS ABDOMINIS PLANE (TAP)
B – ILIOHYPOGASTRIC AND ILIOINGUINAL NERVE
C – RECTUS SHEATH
D – LATERAL FEMORAL CUTANEOUS NERVE
PART 1: TRANSVERSUS ABDOMINIS PLANE NERVE BLOCK (TAP)
Figure 1-2: Innervation of the anterior and lateral abdominal wall. IH, iliohypogastric nerve; IL, ilioinguinal nerve. General Considerations The ultrasound-guided transversus abdominis plane nerve block, or TAP has become a commonly used regional anesthesia technique for a variety of indications. It is largely devoid of complications and can be performed time-efficiently, either at the beginning or the end of surgery for use as postoperative analgesia. Similar to ilioinguinal and iliohypogastric nerve blocks, the method relies on guiding the needle with ultrasound to the plane between the transversus abdominis and internal oblique muscles, to nerve block the anterior rami of the lower six thoracic nerves (T7-T12) and the first lumbar nerve (L1). Injection of local anesthetic within the TAP potentially can provide unilateral analgesia to the skin, muscles, and parietal peritoneum of the anterior abdominal wall from T7 to L1, although in clinical practice, the extent of the nerve block is variable. Ultrasound Anatomy
Figure 1-3: Schematic representation of the abdominal wall muscles. The anterior abdominal wall (skin, muscles, and parietal peritoneum) is innervated by the anterior rami of the lower six thoracic nerves (T7-T12) and the first lumbar nerve (L1). Terminal branches of these somatic nerves course through the lateral abdominal wall within a plane between the internal oblique and transversus abdominis muscles. This intermuscular plane is called the transversus abdominis plane. Injection of local anesthetic within the TAP can result in unilateral analgesia to the skin, muscles, and parietal peritoneum of the anterior abdominal wall. The exact cephalad-caudad spread and extent of anesthesia and analgesia obtained with the TAP nerve block is variable. This subject is not well researched; the actual coverage is likely dependent on the technique details, place of needle insertion (lateral-medial) and volume of local anesthetic injected. Additionally, the patient’s anatomical characteristics may also influence the spread of the injected solutions. Imaging of the abdominal wall between the costal margin and the iliac crest reveals three muscle layers, separated by a hyperechoic fascia: the outermost external oblique (EOM), the internal oblique (IOM), and the transversus abdominis muscles (TAM) (Figures 1-2 and 1-3). Immediately below this last muscle is the transversalis fascia, followed by the peritoneum and the intestines below, which can be recognized as moving structures because of peristalsis. The nerves of the abdominal wall are not visualized consistently, although this is not necessary to accomplish a nerve block.
Distribution of block
Figure 1-4: Transducer position in the transverse abdominal, at the anterior axillary line, between the costal margin and the iliac crest. The exact distribution of abdominal wall anesthesia following a TAP nerve block has not been well documented or entirely agreed on by practitioners. The most fervent proponents of TAP technique maintain that reliable block of dermatomes T10-L1 can be achieved with moderate volumes of local anesthetic (e.g., 20-25 mL). Claims of block up to T7 after single injection of large volume have been made, but these results are not consistently reproduced in clinical practice. In our practice, some TAP nerve blocks have resulted in complete anesthesia for inguinal herniorrhaphy; at other times, the results have been less consistent. Additional research is indicated to clarify the spread of anesthesia and factors that influence it. Equipment Equipment needed includes the following:
Figure 1-5(A) Ultrasound anatomy of the abdominal wall layers. (B) Labeled ultrasound anatomy of the abdominal wall layers, EOM, external oblique muscle; IOM, internal oblique muscle; TAM, transverse abdominis muscle. Landmarks and Patient Positioning This nerve block typically is performed with the patient in the supine position. The iliac crest and costal margin should be palpated and the space between them in the mid-axillary line (usually 8-10 cm) identified as the initial transducer location. The nerve block is almost always performed under general anesthesia in pediatric patients; a common option for adults as well.
Technique
Figure 1-6: Innervation of the anterior and lateral abdominal wall. IH, iliohypogastric nerve; IL, ilioinguinal nerveSimulated needle insertion (1) and distribution of LA (blue shaded area) to accomplish transversus abdominis plane (TAP) nerve block. Shown are the external oblique muscle (EOM), internal oblique muscle (IOM), and the transverse abdominal muscle (TAM). Needle tip is positioned in the tissue sheath between IOM and TAM. With the patient supine, the skin is disinfected and the transducer placed on the skin (Figure 1-4). The three muscle layers should be identified (Figures 1-5A and B). Sliding the transducer slightly cephalad or caudad will aid the identification. Once the transverse abdominal plane is identified, a skin wheal is made 2 to 3 cm medial to the medial aspect of the transducer, and the needle is inserted in-plane in a medial to lateral orientation (Figures 1-1A and 1-6). The needle is guided through the subcutaneous tissue, EOM, and IOM. A “pop” may be felt as the needle tip enters the plane between the two muscles. After gentle aspiration, 1 to 2 mL of local anesthetic is injected to verify the location of the needle tip (Figure 1-6). When injection of the local anesthetic appears to be intramuscular, the needle is advanced or withdrawn carefully 1 to 2 mm and another bolus is administered. This gesture is repeated until the correct plane is achieved. In an adult patient, 20 mL of local anesthetic per side is usually sufficient for successful block. We most commonly use ropivacaine 0.25%. In children, a volume of 0.4 mL/kg per side is adequate for effective analgesia when using ultrasound guidance.
   PART 2: ULTRASOUND-GUIDED ILIOHYPOGASTRIC AND ILIOINGUINAL NERVE BLOCKS General Considerations Ilioinguinal and iliohypogastric nerves are contained in a well- defined tissue plane between the transversus abdominis and internal oblique muscles. The ability to easily image the musculature of the abdominal wall makes blocking these two nerves much more exact than the ‘feel-based’ blind technique.
Figure 2-1: (A) Ultrasound anatomy of the iliohypogastric and ilioinguinal nerve. (B) Labeled ultrasound anatomy of the iliohypogastric and ilioinguinal nerve, ASIS, anterior superior iliac spine; EOM, external oblique muscle; IOM, internal oblique muscle; TAM, transverse abdominal muscle; IiN, ilioinguinal nerve; IhN, iliohypogastric nerve. Ultrasound Anatomy Imaging of the abdominal wall medial and superior to the ASIS reveals three muscle layers, separated by hyperechoic fascia: the outermost external oblique (EOM), the internal oblique (IOM), and the transversus abdominis muscles (TAM) (Figures 2-1A and B). Immediately below transversus abdominus muscle is the fascia transversalis, located just above the peritoneum and the abdominal cavity below, easily recognized as moving structures due to peristalsis. The hyperechoic osseous prominence of the anterior-superior iliac spine (ASIS) is a useful landmark which can be used as a reference, and is seen on the lateral side of the US image in Figure 2-1. The iliohypogastric and ilioinguinal nerves pierce the TAM above the ilium and lie in the plane between the TAM and the IOM. They are often seen side by side or up to 1 cm apart, and they typically appear as hypoechoic ovals. Use of color Doppler may be useful to identify the deep circumflex iliac artery, which lies adjacent to the nerves in the same plane as an additional landmark useful in identifying the nerves. Distribution of block Block of the iliohypogastric and ilioinguinal nerves results in anesthesia of the hypogastric region, the inguinal crease, the upper medial thigh, the mons pubis, part of the labia, the root of the penis, and the anterior part of the scrotum. There is considerable variation in sensory distribution between individuals. Equipment Equipment needed includes the following:
Landmarks and Patient Positioning
Figure 2-2: Transducer position to image the ilioinguinal (IiN) and iliohypogastric nerves (IhN). The transducer is positioned in the immediate vicinity of the anterior superior iliac spine (ASIS). The block of the iliohypogastric and ilioinguinal nerves is done in supine position. Palpation of the ASIS provides the initial landmark for transducer placment. This nerve block is often performed under general anesthesia, particularly in pediatric patients. Technique With the patient supine, the skin is disinfected and the transducer placed medial to the ASIS, oriented on a line joining the ASIS with the umbilicus (Figure 2-2). The three muscle layers should be identified. The nerves should appear as hypoechoic ovals between the IOM and TAM muscles. Moving the transducer slightly cephalad or caudad to trace the nerves can be useful. In addition, color Doppler may be used to attempt to visualize the deep circumflex iliac artery. A skin wheal is made on the medial aspect of the transducer, and the needle is inserted in-plane in a medial to lateral orientation, through the subcutaneous tissue, EOM, and IOM, and is advanced toward the ilioinguinal and iliohypogastric nerves (Figure 1-1B and Figure 2-3). A pop may be felt as the needle tip enters the plane between the muscles. After gentle aspiration, 1 to 2 mL of local anesthetic is injected to confirm the needle tip position (Figure 2-4). When injection of the local anesthetic appears to be intramuscular, the needle is advanced or withdrawn carefully 1 to 2 mm and another bolus is administered. This is repeated until the correct needle position is achieved. The nerve block can be done either with in-plane or out-of-plane needle insertion. In an adult patient, 10 mL of local anesthetic per side is usually sufficient for successful block. In children, a volume of 0.15 mL/kg per side (ropivacaine 0.5%) is adequate for effective analgesia when using ultrasound guidance.
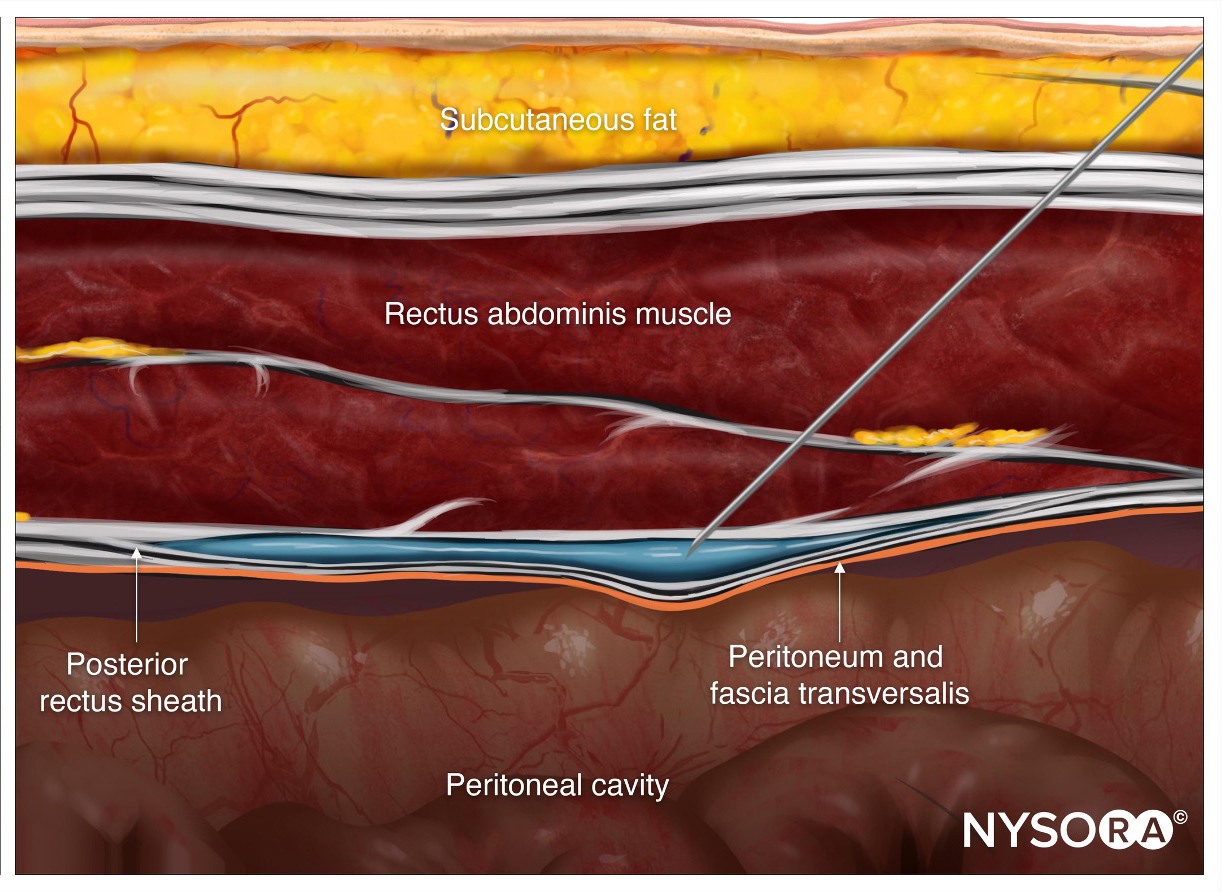
 PART 3: ULTRASOUND-GUIDED RECTUS SHEATH NERVE BLOCK General Considerations The rectus sheath nerve block is a useful technique for umbilical surgery, particularly in pediatric patients. Ultrasound guidance allows for a greater reliability in administering local anesthetic in the correct plane and decreasing the potential for complications. The placement of the needle is in the proximity to the peritoneum and the epigastric arteries. Guiding the needle under ultrasound guidance to the posterior rectus sheath rather than relying on ‘pops’ such as in the traditional, non-ultrasound techniques, makes this nerve block more reproducible and reduces the risk of inadvertent peritoneal and vascular punctures. Ultrasound Anatomy The rectus abdominis muscle is oval shaped, positioned under the superficial fascia of the abdomen. Laterally, the aponeurosis of the external oblique, internal oblique and transversus abdominis muscles split to form two lamellae that surround the muscle anteriorly and posteriorly (forming the rectus sheath), before rejoining again in the midline to insert on the linea alba (Figures 3-1A and B). The 9th, 10th, and 11th intercostal nerves are located in the space between the rectus abdominis muscle and its posterior rectus sheath, although they are usually difficult to depict sonographically. Color Doppler reveals small epigastric arteries in the same plane. Deep to the rectus sheath is preperitoneal fat, peritoneum, and abdominal content (bowel), which can usually be observed moving with peristalsis. Distribution of block block of the nerves of the rectus sheath results in anesthesia of the periumbilical area (spinal dermatomes 9, 10, and 11). It is a rather specific, limited region of block, hence its specific indications.
Figure 3-1: (A) Ultrasound anatomy of the rectus abdominis sheath. (B) Labeled Ultrasound anatomy of the rectus abdominis sheath. RAM, rectus abdominis muscle.
Figure 3-2: Transducer position and needle insertion to accomplish rectus sheath nerve block. Equipment Equipment needed includes the following:
Landmarks and Patient Positioning Typically this nerve block is performed in the supine position.
Technique With the patient in supine position, the skin is disinfected and the transducer placed at the level of the umbilicus immediately lateral, in transverse position (Figure 3-2). Color Doppler can be used to identify the epigastric arteries so that their puncture can be avoided. The needle is inserted in-plane in a medial to lateral orientation, through the subcutaneous tissue, to pearce through the anterior rectus sheath (Figure 3-3). Out-of-plane technique is also suitable and often preferred in obese patients. The needle is further advanced through the body of the muscle until the tip rests on the posterior rectus sheath. After negative aspiration, 1 to 2 mL of local anesthetic is injected to verify needle tip location (Figure 3-4). When injection of the local anesthetic appears to be intramuscular, the needle is advanced 1 to 2 mm and its position is checked by injection of another aliquot of local anesthetic. This is repeated until the correct needle position is achieved. When a large volume of local anesthetic is planned (e.g. in combining billateral TAP and rectus abdominis sheath nerve blocks), the described “hydrodisection” for the purpose of localization of the needle tip can be done using 0.9% saline or chlorprocaine to decrease the total mass of the more toxic, longer acting local anesthetic. In an adult patient, 10 mL of local anesthetic (e.g., 0.5% ropivacaine) per side is usually sufficient for successful block. In children, a volume of 0.1 mL/kg per side is adequate for effective analgesia.
 PART 4: ULTRASOUND-GUIDED LATERAL FEMORAL CUTANEOUS NERVE BLOCK General Considerations
Figure 4-1: Cross-sectional anatomy of the lateral femoral cutaneous nerve (LFCN). Shown are LFCN, sartorius muscle (SaM), and tensor fascia latae muscle (TFLM). The lateral femoral cutaneous nerve (LFCN) divides into approximately two to five branches innervating the lateral and upper aspects of the thigh. Many studies have described how the variable anatomy of the lateral femoral cutaneous nerve makes it challenging to perform an effective landmark-based technique nerve block. Ultrasound guidance, however, allows more accurate needle insertion into the appropriate fascial plane where lateral femoral cutaneous nerve passes through, allowing for a higher success rate. Ultrasound Anatomy The lateral femoral cutaneous nerve typically is located between the tensor fasciae latae (TFLM) and sartorius (SaM) muscles, 1 to 2 cm medial and inferior to the anterior superior iliac spine (ASIS) and 0.5 to 1.0 cm deep to the skin surface (Figure 4-1). Ultrasound imaging of the lateral femoral cutaneous nerve yields an oval hypoechoic structure in cross-sectional view. The lateral edge of the sartorius muscle is a useful landmark, and as such, it can be relied on throughout the procedure. (Figures 4-2A and B). The LFCN branches sometimes may be seen across the anterior margin of the TFL. Distribution of block Block of the lateral femoral cutaneous nerve provides anesthesia or analgesia in the anterolateral thigh. There is a large variation in the area of sensory coverage among individuals because of the highly variable course of LFCN and its branches.
Figure 4-2: (A) Ultrasound anatomy of the lateral femoral cutaneous nerve (LFCN). (B) Labeled ultrasound anatomy of the LFCN. Equipment Equipment needed includes the following:
Landmarks and Patient Positioning Block of the lateral femoral cutaneous nerve is performed with the patient in the supine or lateral position. Palpation of the anterior-superior spine provides the initial landmark for transducer placement; the transducer is first positioned at 2 cm inferior and medial to the ASIS and adjusted accordingly. Typically, the nerve is identified slightly more distally in its course. If nerve stimulator is used, precise identification of the LFCN may be confirmed by eliciting a tingling sensation on the lateral side of the thigh.
Technique
Figure 4-3: Transducer position and needle insertion to accomplish a lateral femoral cutaneous nerve (LFCN) block. With the patient supine, the skin is disinfected and the transducer placed immediately inferior to the ASIS, parallel to the inguinal ligament (Figure 4-3). The tensor fasciae latae and the sartorius muscle should be identified. The nerve should appear as a small hypoechoic oval structure between the tensor fasciae latae and the sartorius muscle in a short- axis view. A skin wheal is then made on the lateral aspect of the transducer, and the needle is inserted in-plane in a lateral to medial orientation, through the subcutaneous tissue and the tensor fasciae latae muscle (Figure 4-4A). A pop may be felt as the needle tip enters the plane between the tensor fascia latae and sartorius muscles. After gentle aspiration, 1 to 2 mL of LA is injected to verify the needle tip position. When the injection of the LA appears to be intramuscular, the needle is withdrawn or advanced 1 to 2 mm and another bolus is administered. This is repeated until the correct position is achieved by visualizing the spread of the LA in the described plane between the tensor fasciae latae and sartorius muscles (Figure 4-4B). In an adult patient, 5 to 10 mL of LA is usually sufficient for successful block. In children, a volume of 0.15 mL/kg per side is adequate for effective analgesia.
Figure 4-4: (A) Simulated needle path (1) to nerve block the LCFN. (B) Simulated needle path (1) and local anesthetic spread (area shaded in blue) to anesthetize the LFCN.
 |

Explore NYSORA knowledge base for free:


 A
A B
B
 A
A B
B
 A
A B
B