Goal
Identify pericardial effusion or tamponade.
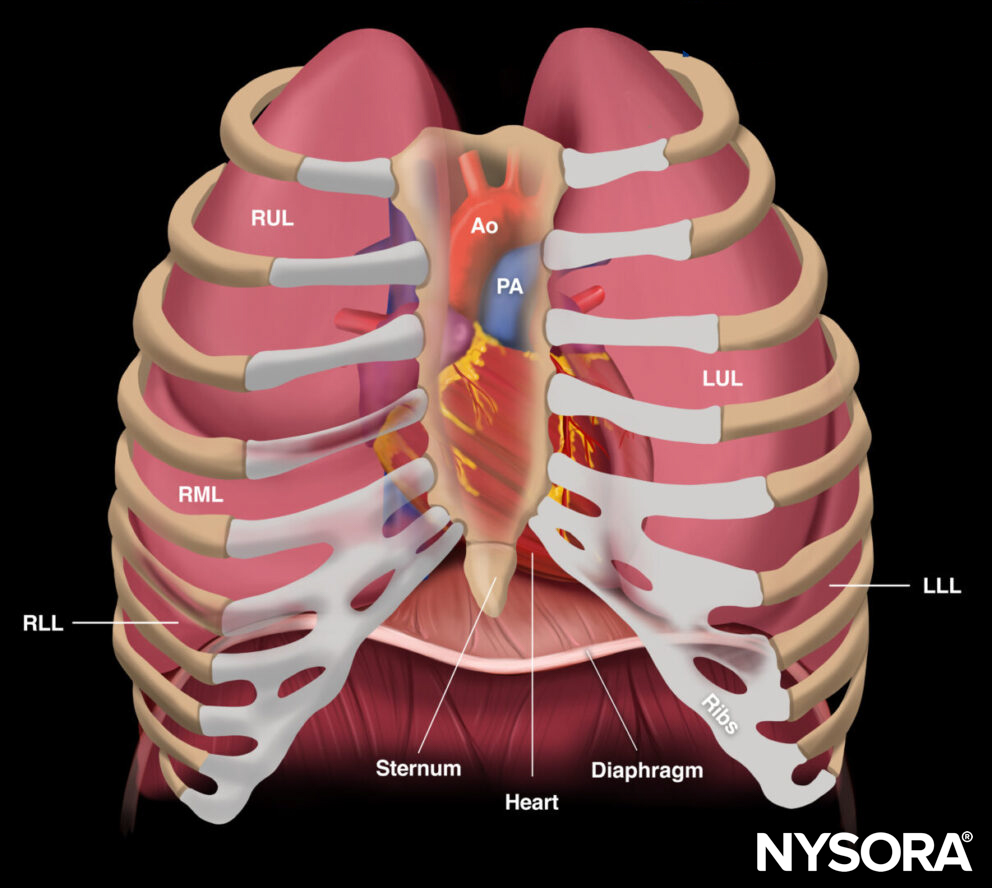
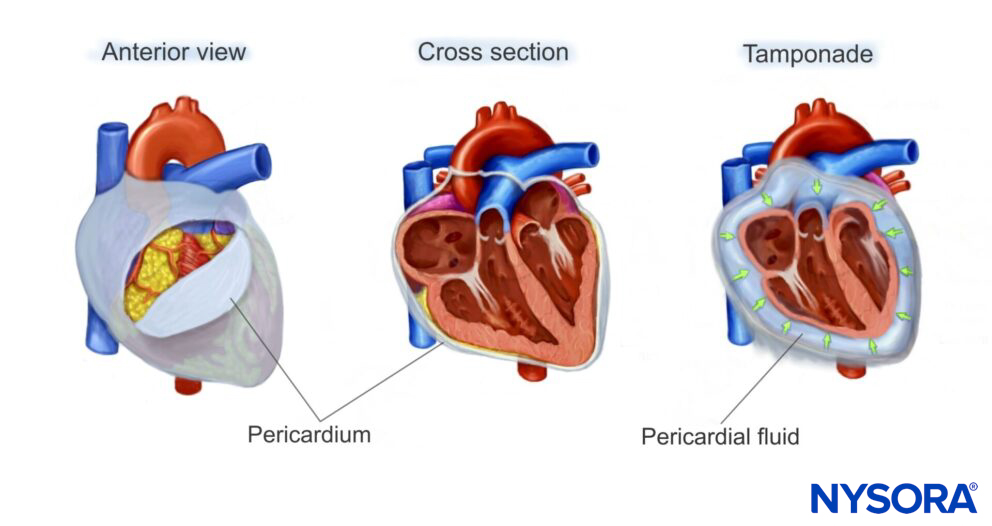
The pericardium is a virtual space that surrounds the heart. It consists of two layers:
- The inner visceral pericardium
- The outer parietal pericardium
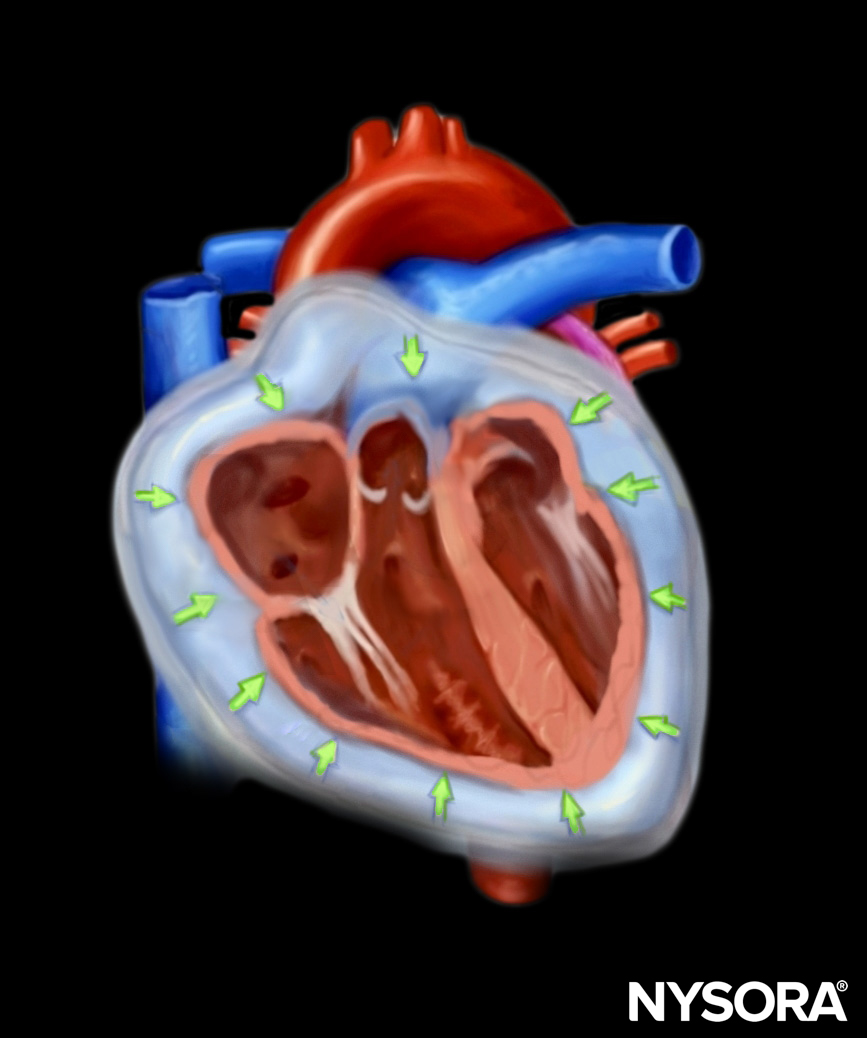
Fluid can collect between these layers due to medical or surgical conditions. When pericardial fluid compresses the heart and reduces the cardiac output, it is called a tamponade.
Fluid can collect in the pericardial space, decreasing cardiac output by interfering with cardiac filling.
The fluid can be:
- Transudative
- Exudative
- Hemorrhagic
- Malignant
The onset of a pericardial effusion can be either rapid or slow. A slow effusion is better tolerated in terms of pericardial volume, but when intrapericardial pressure reaches a threshold, right ventricular filling is compromised, and tamponade ensues. This is usually when the limit of pericardial stretch is reached.

The effect of rapid and slow effusion on the intrapericardial pressure and volume of pericardial fluid.
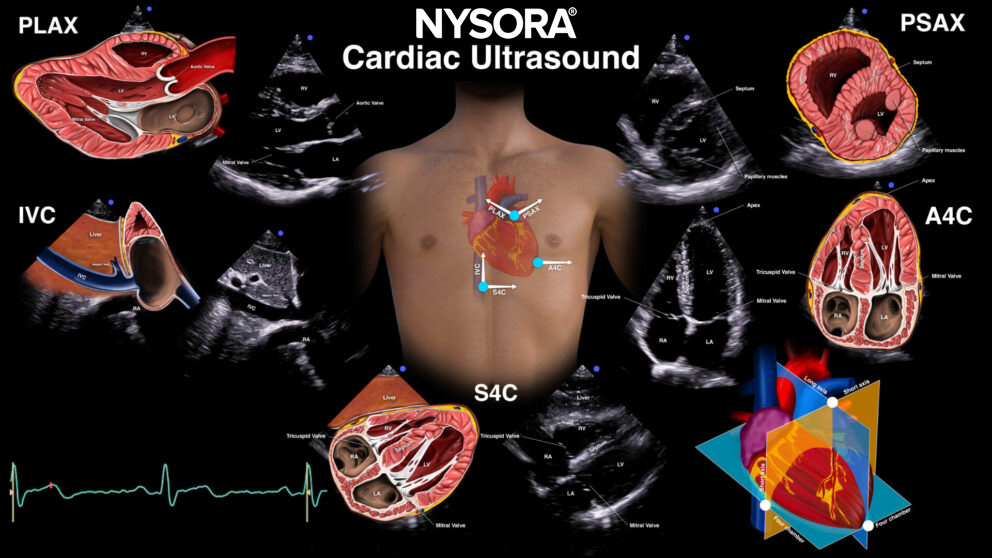
Views
Subcostal four-chamber view (S4C)

Transducer position and sonoanatomy of the subcostal four-chamber view.
Parasternal long-axis view (PLAX)
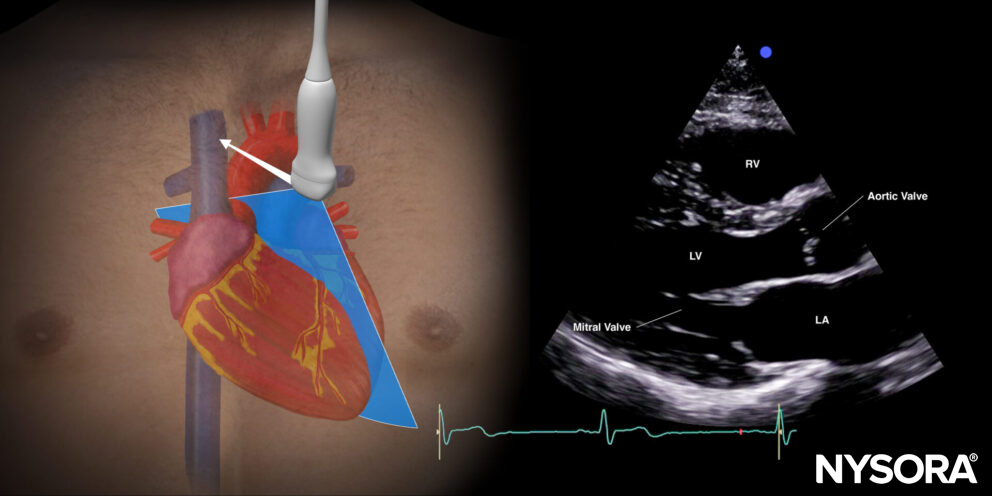
Transducer position and sonoanatomy of the parasternal long-axis view.
Parasternal short-axis view (PSAX)
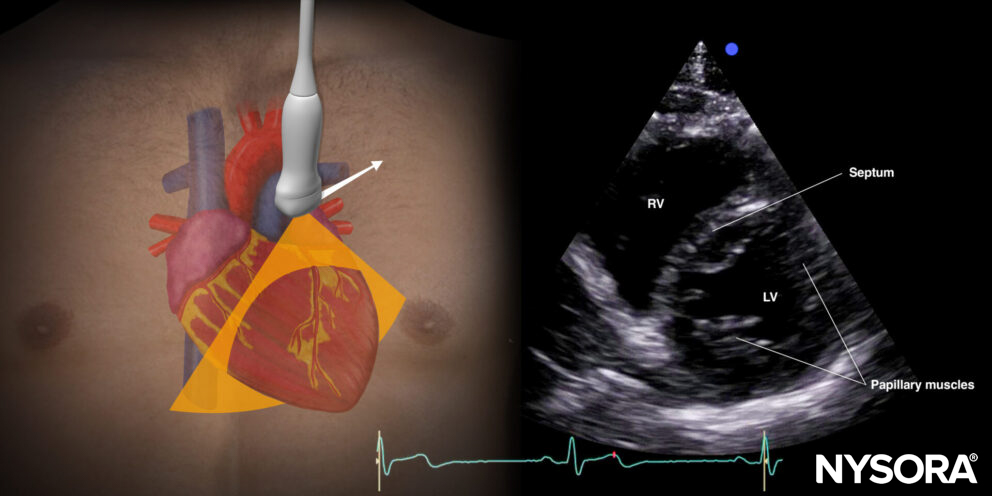
Transducer position and sonoanatomy of the parasternal short-axis view.
Apical four-chamber view (A4C)
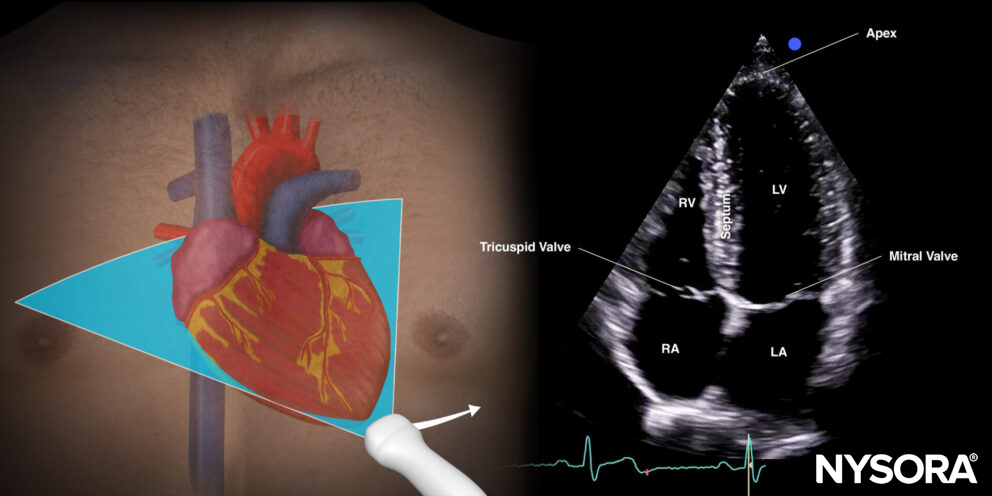
Transducer position and sonoanatomy of the apical four-chamber view.
Inferior vena cava view (IVC)
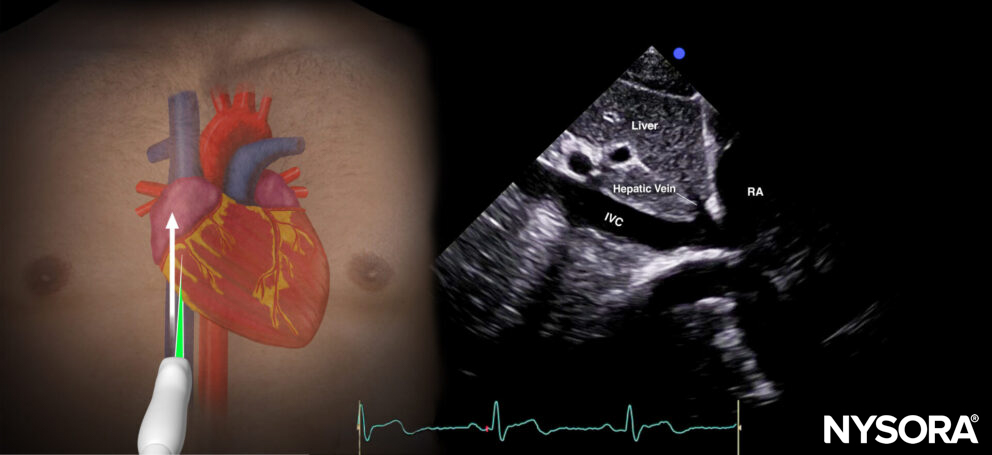
Transducer position and sonoanatomy of the inferior vena cava view.
Assessment
Ultrasound features: Anechogenic layer between the heart and the pericardium:
- Size: Measure at end-diastole! (overestimation during systole)
- Small: < 1 cm
- Moderate: 1-2 cm
- Large: > 2 cm
- Cardiac cycle:
- Only during systole: Small
- During systole and diastole: Moderate – large
- Location:
- Posterior or inferior: Small
- Circumferential: Moderate – large
- Dilated inferior vena cava without respiratory variation in case of tamponade: >2cm.
- Compression of the right atrium and right ventricle during diastole: more likely to result in tamponade.
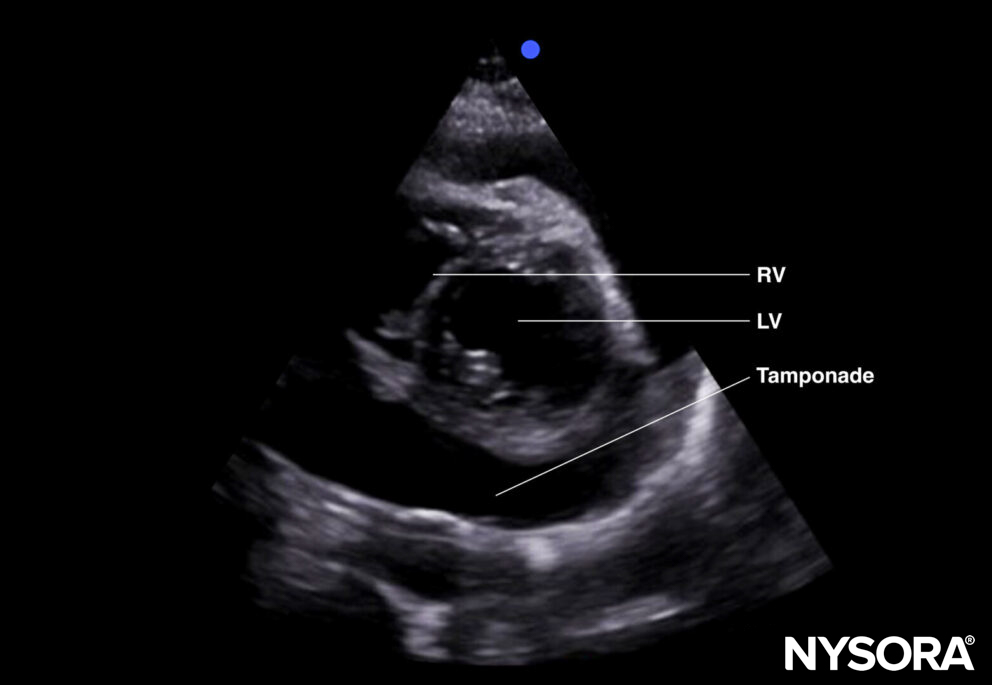
Tamponade (parasternal short-axis view).
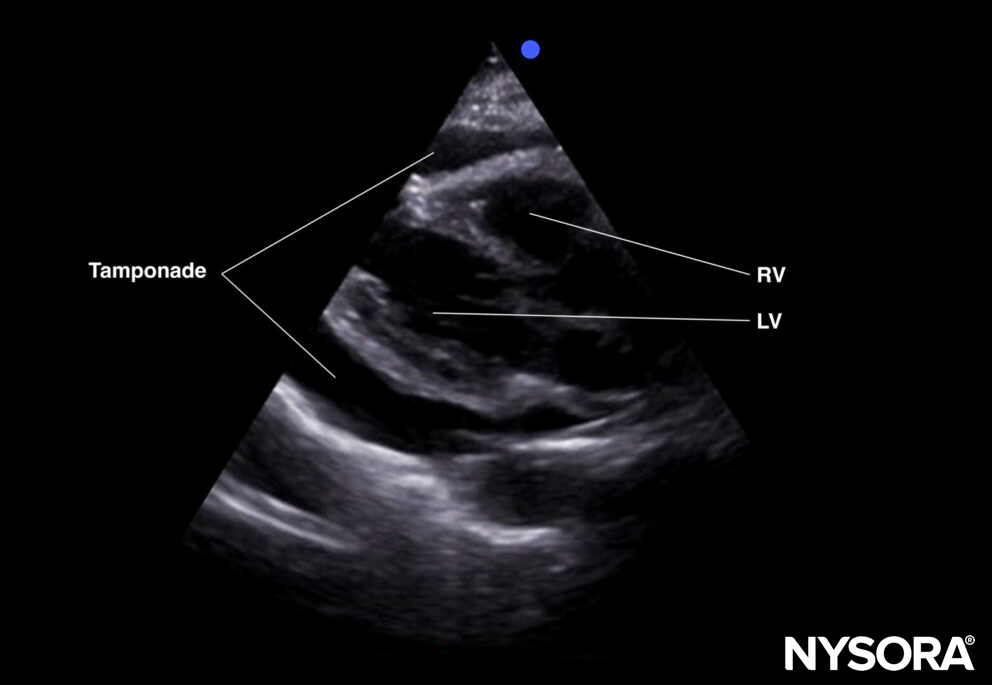
Tamponade (parasternal long-axis view).
Tips
- The size of the pericardial effusion does not necessarily correlate with the hemodynamics.
- The clinical presentation of the tamponade gives you an idea about the severity of the tamponade:
- Cardiac arrest or deep circulatory shock: Urgent pericardiocentesis or cardiac surgery is needed.
- Moderate hypotension, pulsus paradoxus: Administer IV fluids and consult cardiology.
- False negative results may be due to echogenic effusions (thrombi, pus) or loculated effusions (adhesions, malignancy).
- Fat pads on the myocardium can result in a false positive diagnosis. Usually, they move with the myocardium and are more heterogeneous on ultrasound.
- When it is difficult to differentiate pleural from pericardial effusion, use the parasternal long-axis view to locate the fluid in relation to the descending thoracic aorta and the pericardium. The descending aorta can be found posterior to the heart.
- Anterior/superficial to the descending aorta and the pericardium: Pericardial effusion.
- Posterior/deep to the descending aorta and the pericardium: Pleural effusion.
Clinical updates
Alerhand et al. (American Journal of Emergency Medicine, 2022) provide a comprehensive emergency medicine review of pericardial tamponade emphasizing bedside echocardiography, noting that classic Beck’s triad is infrequent (hypotension present in only 14–35%) and that ultrasound findings, particularly diastolic RV collapse (48–60% sensitive, 75–90% specific), systolic RA collapse (up to 100% sensitive as disease progresses), plethoric non-collapsible IVC (95–97% sensitive), and >30% respiratory variation in mitral inflow, are central to diagnosis. They stress that POCUS shortens time to diagnosis and pericardiocentesis, recommend dynamic assessment of chamber collapse timing, and outline ultrasound-guided drainage principles (largest, shallowest pocket; real-time needle visualization; agitated saline confirmation) to reduce complication rates (0.5–3.7% with ultrasound vs 15–20% blind).
- Alerhand S, Adrian RJ, Long B, Avila J. Pericardial tamponade: A comprehensive emergency medicine and echocardiography review. Am J Emerg Med. 2022;58:159-174.