Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About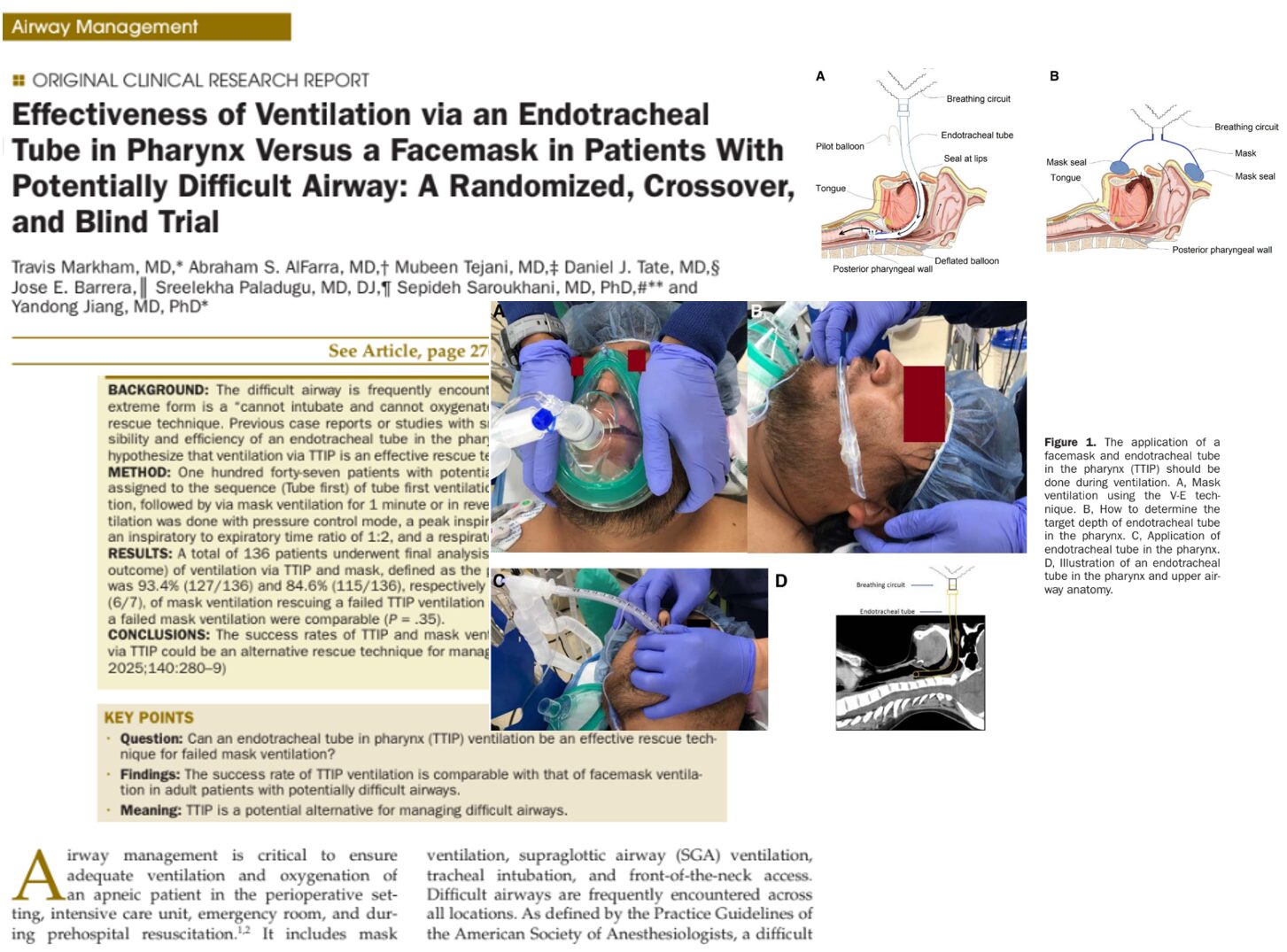





Managing a difficult airway is one of the most critical and high-stakes challenges in anesthesia and emergency care. A new study by Markham et al. has found that a lesser-known method, ventilation via an endotracheal tube placed in the pharynx (TTIP), is a viable rescue technique when traditional facemask ventilation fails.
Why difficult airway management matters
Airway management is a cornerstone of anesthesia and emergency care. In critical moments, failure to secure an airway can lead to hypoxia, brain injury, or death. The most feared scenario is the “cannot intubate, cannot oxygenate” (CICO) event, a rare but catastrophic condition with mortality rates up to 50% in emergency settings.
Standard rescue methods such as mask ventilation, supraglottic airway (SGA) devices, or surgical airway techniques often fall short:
- Facemask ventilation: Prone to failure in obese patients or those with facial anomalies.
- SGAs: Variable success rates and are not always effective in prehospital settings.
- Surgical airway: Invasive, requires high skill, and has success rates as low as 35% even among anesthesiologists.
Hence, the exploration of TTIP, a low-tech, potentially lifesaving option, offers new hope.
What is TTIP ventilation?
TTIP involves inserting an uncuffed endotracheal tube blindly into the pharynx, stopping short of the vocal cords. It’s designed to bypass obstructions caused by the tongue, soft palate, and epiglottis, common culprits of failed ventilation during anesthesia.
How it works:
- Positive pressure ventilation is delivered directly into the pharynx.
- The tube acts as a stent, keeping the upper airway open.
- Airflow is directed closer to the glottis, minimizing dead space and overcoming upper airway collapse.
Key findings from the study
Study design:
- Type: Prospective, randomized, crossover, and blinded clinical trial
- Sample: 147 adult patients with potentially difficult airways
Primary outcome:
Success was defined as visible end-tidal CO₂ within the first three breaths.
Success rate:
- TTIP: 93.4% (127/136)
- Mask ventilation: 84.6% (115/136)
- TTIP successfully rescued 100% of failed mask cases.
- Mask rescued 85.7% of failed TTIP cases.
- Only 1 out of 136 patients (0.7%) failed both methods.
Additional data points:
- End-tidal CO₂ (ETCO₂) was significantly higher with TTIP (mean 34.4–36.4 mm Hg vs. 32.7–33.9 mm Hg).
- Expired oxygen fraction (FeO₂) showed no significant difference between TTIP and mask.
- Expired tidal volume was higher with the mask (701.5 mL vs. 611.1 mL), but TTIP had less mechanical dead space.
TTIP vs. current rescue methods
Supraglottic airways (SGAs):
- Perioperative rescue rate: ~63%
- Prehospital first-attempt success: ~83%
- Success after 3 attempts: ~64%
In comparison, TTIP:
- Achieved 100% rescue success in this trial
- Requires no specialized equipment
- Has a rapid learning curve—even novice providers succeeded after minimal training
How to perform TTIP ventilation
Equipment:
- 7.0–8.0 mm endotracheal tube
- Operating room ventilator or manual resuscitator
Steps:
- Determine insertion depth: Measure the distance from the ear canal to the upper incisors.
- Insert the tube:
- Use the natural curvature of the tube aligned with the tongue.
- Gently advance without forcing.
- Create a seal:
- Use a two-handed technique at the lips.
- If needed, pinch the nose to prevent leaks.
- Start ventilation:
- Set the ventilator to pressure control mode.
- Use 20 cm H₂O peak inspiratory pressure, 1:2 I:E ratio, 10 breaths/min.
- Confirm success:
- Look for three-phase ETCO₂ on capnography.
Benefits of TTIP ventilation
- Non-invasive and equipment-light
- No need for cuff inflation
- Effective even with facial trauma or beards
- Not dependent on head elevation or ideal positioning
- Can be used in conjunction with or while preparing for a surgical airway
Conclusion: a new tool in the airway arsenal
Ventilation using an endotracheal tube in the pharynx (TTIP) is a viable and effective method for managing difficult airways, particularly when mask ventilation fails. Its simplicity, accessibility, and high success rate suggest it may soon become an essential skill in both routine and emergency airway management.
Next steps:
Larger, multicenter trials comparing TTIP to facemask with airway adjuncts and SGAs are warranted. With evidence growing, TTIP could be formally integrated into difficult airway algorithms worldwide.
Reference: Markham T. et al. Effectiveness of Ventilation via an Endotracheal Tube in Pharynx Versus a Facemask in Patients With Potentially Difficult Airway: A Randomized, Crossover, and Blind Trial. Anesth Analg. 2025;140:280-289.
For more information on this topic, check out Anesthesia Updates on the NYSORA Anesthesia Assistant App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights, all in one place. Download the app today and experience the future of anesthesia education and decision-making.