Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About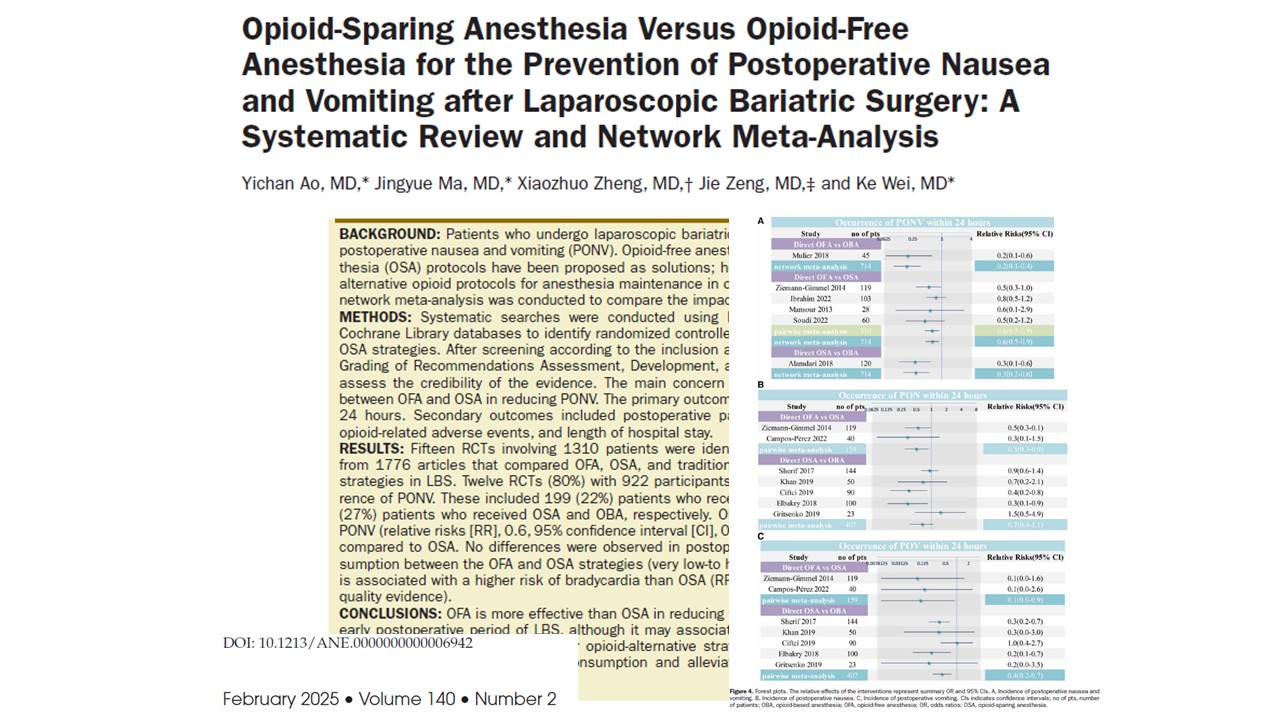





The systematic review and meta-analysis by Yichan et al. 2025 published in Anesthesia & Analgesia evaluates the effectiveness of opioid-free anesthesia (OFA) and opioid-sparing anesthesia (OSA) in preventing postoperative nausea and vomiting (PONV) after laparoscopic bariatric surgery (LBS). With 15 randomized controlled trials (RCTs) and 1,310 patients analyzed, this study sheds light on how different anesthesia strategies impact PONV, pain control, and recovery in obese patients.
Key findings
- Opioid-Free anesthesia (OFA) significantly reduces PONV
- OFA reduced the risk of PONV more effectively than OSA (RR 0.6, 95% CI: 0.5–0.9).
- The incidence of PONV was lowest in OFA, followed by OSA, and highest in traditional opioid-based anesthesia (OBA).
- OFA was superior in preventing postoperative vomiting (POV) and had a modest effect on nausea reduction.
- No significant difference in postoperative pain control
- OFA and OSA effectively managed pain, showing no significant differences in postoperative pain scores.
- Patients in the OFA and OSA groups required fewer opioids for postoperative pain relief compared to OBA.
- At 24 hours post-surgery, patients who received OFA or OSA had lower pain scores compared to traditional opioid anesthesia.
- OFA and OSA lead to lower postoperative opioid consumption
- Both opioid-alternative strategies significantly reduced opioid use in the postanesthesia care unit (PACU).
- No significant differences in opioid consumption were observed between OFA and OSA over the first 24 hours.
- Increased risk of bradycardia with OFA
- Patients receiving OFA had a higher incidence of bradycardia (RR 2.6, 95% CI: 1.2–5.9).
- OSA had the lowest risk of bradycardia, followed by OBA and OFA.
- There is no significant difference in perioperative hypotension between OFA and OSA.
- No significant impact on hospital length of stay (LOS)
- LOS was similar across all anesthesia strategies, suggesting that OFA or OSA do not prolong hospital recovery.
Clinical implications
- Opioid-free anesthesia: A game-changer for PONV reduction
For obese patients undergoing bariatric surgery, PONV is a major concern, affecting up to 70% of cases. This study confirms that eliminating opioids (OFA) is the most effective strategy for PONV prevention, supporting its integration into enhanced recovery after surgery (ERAS) protocols.
- Opioid-sparing strategies are just as effective for pain Relief
- The study shows that reducing or eliminating opioids intraoperatively does not compromise pain management.
- Patients experienced similar pain relief with OFA and OSA, suggesting that opioids are not necessary for effective pain control postoperatively.
- Balancing benefits with risks: bradycardia in OFA
- While OFA significantly reduces PONV, it comes with a higher risk of bradycardia.
- This risk may be attributed to dexmedetomidine, a common component of OFA, which can cause slower heart rates.
- Clinicians should carefully weigh the benefits of PONV reduction against the risks of cardiovascular instability.
4. Tailored anesthesia approaches for obese patients
- The study highlights the need for individualized anesthesia plans, particularly for patients at higher risk of hemodynamic instability.
- For patients with pre-existing cardiac conditions, OSA may be a safer option than OFA.
Conclusion
This comprehensive meta-analysis provides strong evidence that opioid-free anesthesia (OFA) significantly reduces postoperative nausea and vomiting (PONV) compared to opioid-sparing anesthesia (OSA) in bariatric surgery patients. While both strategies effectively reduce opioid use and control pain, OFA carries a higher risk of bradycardia. These findings suggest that OFA may be the preferred approach for PONV prevention, but clinicians should carefully assess patient-specific risks when choosing anesthesia strategies.
What this means for anesthesia practice
- Stronger case for opioid-free anesthesia in ERAS protocols.
- More research is needed to refine opioid-alternative strategies for high-risk patients.
- Potential paradigm shifts away from routine intraoperative opioid use in bariatric surgery.
For more information, refer to the full article in Anesthesia & Analgesia.
Ao Y, Ma J, Zheng X, Zeng J, Wei K. Opioid-Sparing Anesthesia Versus Opioid-Free Anesthesia for the Prevention of Postoperative Nausea and Vomiting after Laparoscopic Bariatric Surgery: A Systematic Review and Network Meta-Analysis. Anesth Analg. 2025 Feb 1;140(2):385-396.
https://journals.lww.com/anesthesia-analgesia/abstract/2025/02000/opioid_sparing_anesthesia_versus_opioid_free.24.aspx
Read about PONV in our Anesthesiology Manual: Best Practices & Case Management. Don’t miss out—get your copy on Amazon or Google Books.