Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About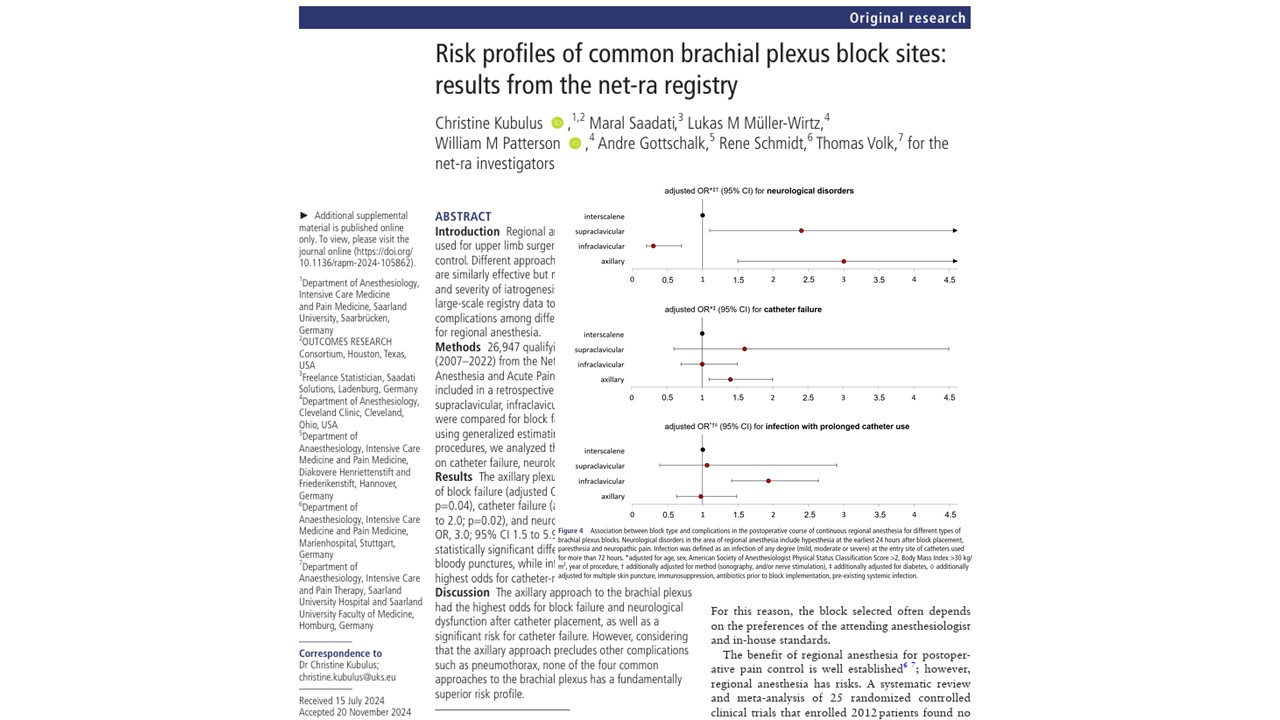





Brachial plexus blocks remain a cornerstone of regional anesthesia for upper extremity surgery and postoperative analgesia. In clinical practice, anesthesiologists commonly choose among four major approaches:
Although these techniques are often considered interchangeable for many surgical procedures, each block site carries distinct anatomical and procedural risks.
A new large multicenter registry analysis published in Regional Anesthesia & Pain Medicine examined whether any brachial plexus block approach demonstrates a superior overall safety profile. The investigators analyzed nearly 27,000 procedures from the German net-ra registry to compare complication rates across the four major approaches.
Methods
Investigators performed a retrospective cohort analysis using data from the “Network for Safety in Regional Anesthesia and Acute Pain Therapy” (net-ra) registry between 2007 and 2022.
The final analysis included:
- 26,947 adult brachial plexus blocks
- 25 participating centers
- More than 22,000 continuous catheter procedures
The four block approaches analyzed were:
- Interscalene: 17,460 blocks
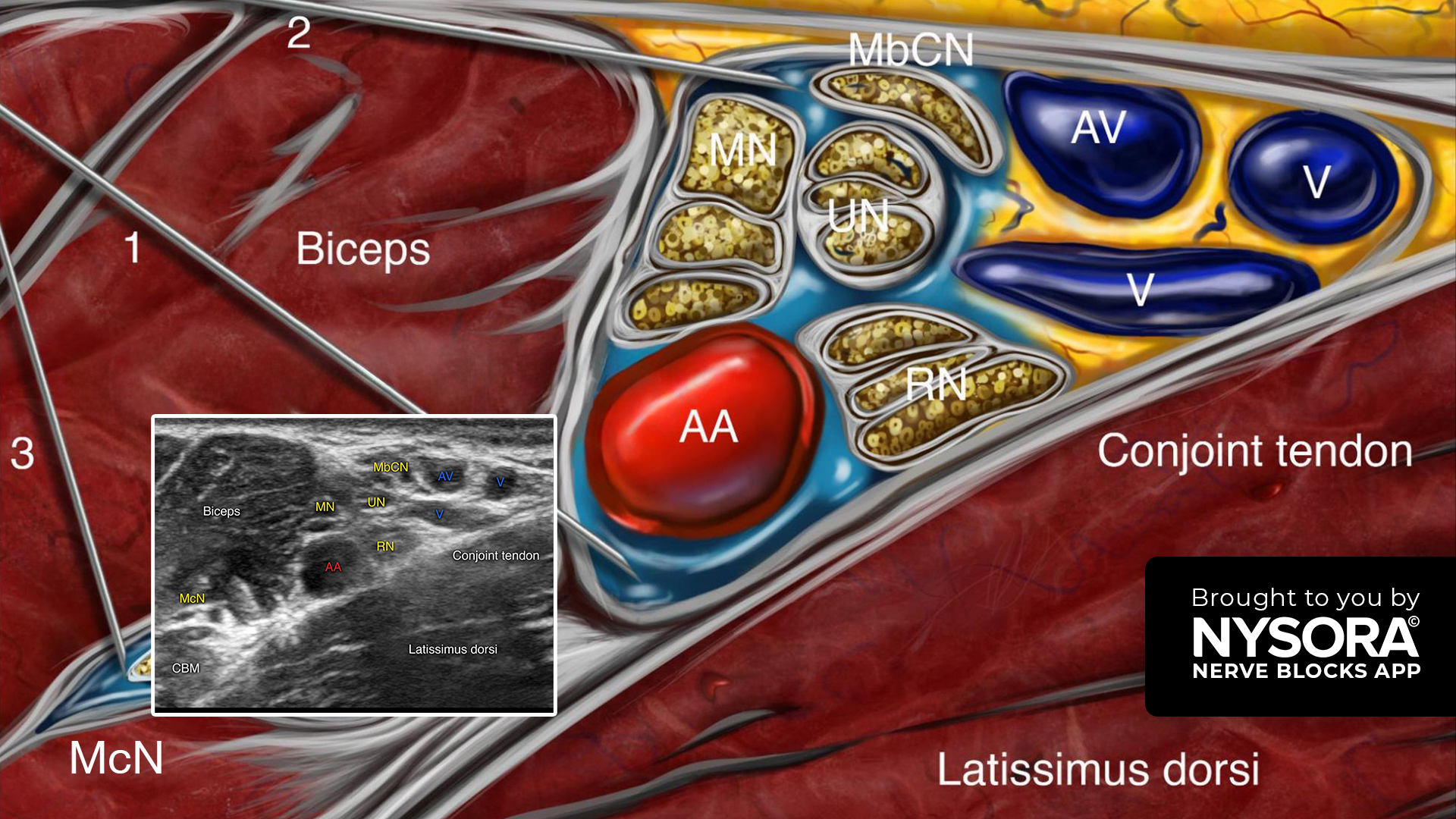
- Axillary: 4,472 blocks
- Infraclavicular: 4,025 blocks
- Supraclavicular: 990 blocks
Researchers evaluated several clinically relevant complications, including:
Procedural complications
- Block failure
- Bloody puncture
- Pneumothorax
- Local anesthetic systemic toxicity (LAST)
Postoperative complications
- Neurological dysfunction
- Catheter failure
- Catheter-related infections
- Respiratory insufficiency
- Horner’s syndrome
The statistical models adjusted for multiple confounders, including:
- Age
- Sex
- BMI
- ASA status
- Ultrasound guidance
- Nerve stimulation
- Antithrombotic therapy
- Diabetes
- Multiple puncture attempts
Key findings
Axillary blocks had the highest failure rates
The axillary approach demonstrated the highest odds of block failure compared with interscalene blocks.
Raw failure rates were:
- Axillary: 17%
- Supraclavicular: 8%
- Interscalene: 4%
- Infraclavicular: 2%
The authors suggested that axillary blocks may be technically more demanding because multiple terminal nerves must be individually identified and anesthetized.
Neurological symptoms were highest with axillary and supraclavicular catheters
Postoperative neurological disorders included:
- Hypesthesia
- Paresthesia
- Neuropathic pain
axillary catheters demonstrated the highest odds of neurological dysfunction: OR=3.0 (95% CI 1.5–5.9)
Supraclavicular catheters also showed increased odds: OR=2.4 (95% CI 1.1–5.6)
In contrast, infraclavicular catheters showed significantly lower odds of neurological complications compared with interscalene approaches.
Importantly, most neurologic symptoms were transient:
- 86% resolved before the end of acute pain service follow-up.
Infraclavicular catheters had the highest infection risk
Among catheters left in place longer than 72 hours, infraclavicular catheters demonstrated the highest adjusted infection risk: OR=1.9 (95% CI 1.4–2.6)
Observed infection rates were:
- Infraclavicular: 7%
- Interscalene: 4%
- Axillary: 4%
- Supraclavicular: 4%
Most infections were classified as mild.
Bloody punctures were uncommon
Bloody punctures occurred infrequently across all approaches: 1%–2%
No statistically significant difference was observed among block sites after adjustment.
Serious complications were rare
Severe complications remained uncommon throughout the registry:
- Only four plausible pneumothoraces were documented
- Only two cases of LAST were reported
- Horner’s syndrome occurred exclusively with interscalene blocks
- Respiratory insufficiency was most common with the interscalene approach
Results interpretation
The study highlights that each brachial plexus approach has its own characteristic pattern of complications rather than demonstrating universally superior safety.
Axillary approach
Advantages:
- Avoids pneumothorax
- Avoids phrenic nerve paresis
Disadvantages:
- Highest block failure rates
- Highest neurological complication rates
- Increased catheter failure
Interscalene approach
Advantages:
- Reliable proximal coverage
- Lower failure rates
Disadvantages:
- Respiratory complications
- Horner’s syndrome
- Diaphragmatic involvement
Infraclavicular approach
Advantages:
- Lowest neurological complication rates
- Low block failure rates
Disadvantages:
- Highest catheter infection rates
Supraclavicular approach
Advantages:
- Dense upper extremity anesthesia
- Broad surgical applicability
Disadvantages:
- Increased neurological symptom risk
- Potential thoracic complications
The investigators concluded that no single brachial plexus block approach demonstrated a fundamentally superior overall risk profile.
Limitations
The authors acknowledged several important limitations.
Retrospective registry design
The study relied on routine clinical documentation, which introduces potential risks of underreporting and missing data.
No long-term neurologic follow-up
Follow-up was limited to the inpatient acute pain service period. Long-term neurologic outcomes were not available.
Evolving practice patterns
The study period spanned 15 years, during which ultrasound guidance and regional anesthesia techniques evolved substantially.
Residual confounding
As with all observational studies, unmeasured confounders may still have influenced outcomes.
Practical tip
This study reinforces that brachial plexus block selection should remain individualized rather than protocol-driven.
When choosing a block approach, clinicians should consider:
- Surgical location
- Respiratory reserve
- Patient comorbidities
- Anticoagulation status
- Catheter duration
- Provider expertise
- Institutional experience
Importantly, no approach should be automatically considered the “safest” in all clinical situations.
The safest block is often the one best matched to the patient, the procedure, and the operator’s expertise.
For more information, refer to the full article in RAPM.
Kubulus C, Saadati M, Müller-Wirtz LM, Patterson WM, Gottschalk A, Schmidt R, Volk T; net-ra investigators. Risk profiles of common brachial plexus block sites: results from the net-ra registry. Reg Anesth Pain Med. 2026 Apr 2;51(4):443-453.
Download the Nerve Blocks App HERE for brachial plexus blocks. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format – an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Module on NYSORA360!