Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About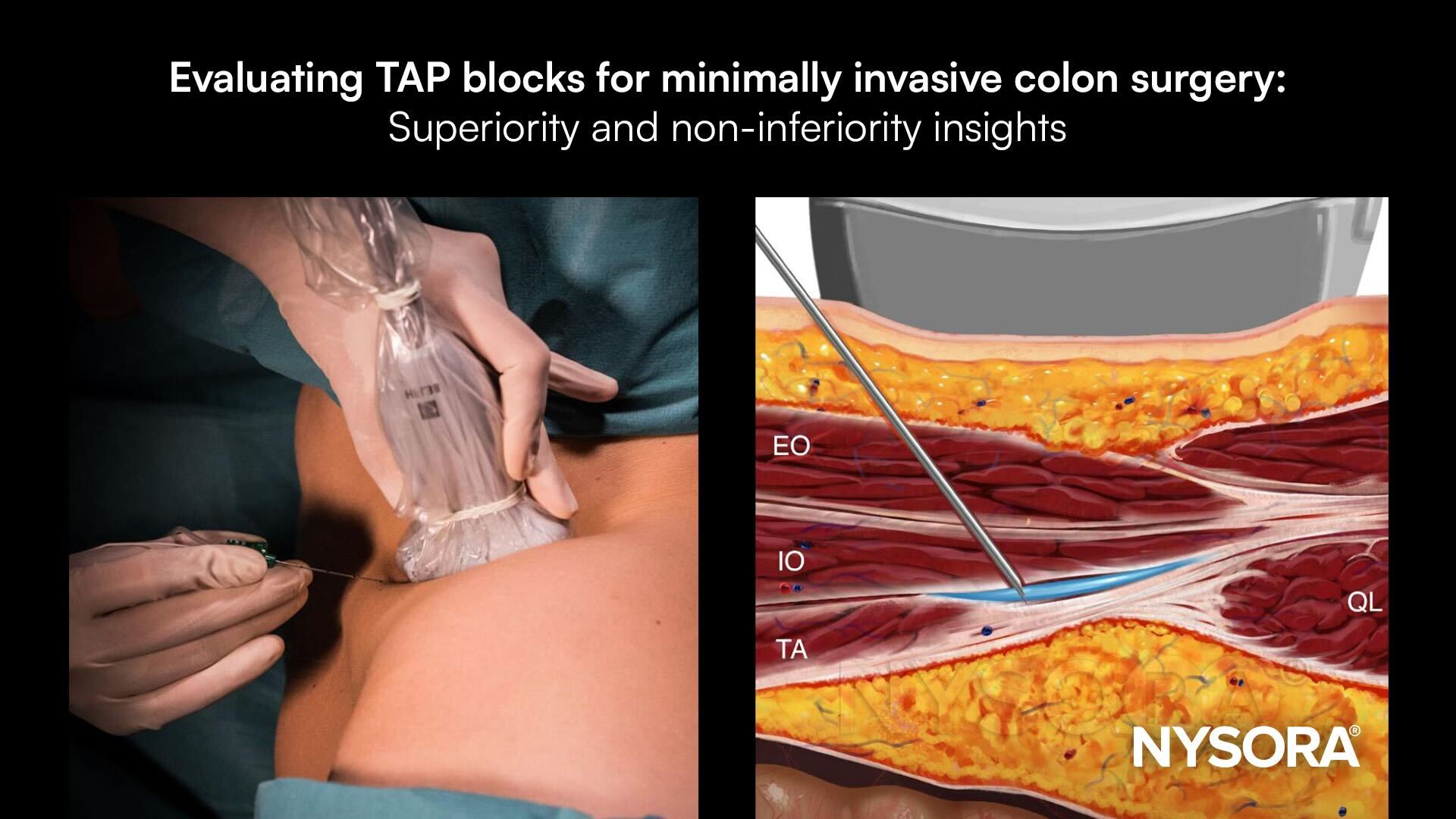





Enhanced recovery after surgery (ERAS) protocols are the gold standard for colorectal surgeries, prioritizing effective pain management to minimize opioid use and complications. The transversus abdominis plane (TAP) block is widely used, but its clinical relevance in minimally invasive colon surgery remains debated. A multicenter, three-arm randomized controlled trial evaluated the efficacy of ultrasound-guided (US-TAP) and laparoscopic-assisted (L-TAP) TAP blocks compared to placebo, with the secondary aim of assessing whether L-TAP is non-inferior to US-TAP.
Study objective and methods
The primary objective was to compare morphine equivalent consumption within 24 hours postoperatively across three groups: US-TAP, L-TAP, and placebo. Secondary objectives included quality of recovery and postoperative pain scores.
-
- Participants: The trial enrolled 340 patients undergoing minimally invasive colon surgery, randomized into US-TAP (127), L-TAP (127), and placebo (86) groups.
- Block techniques:
-
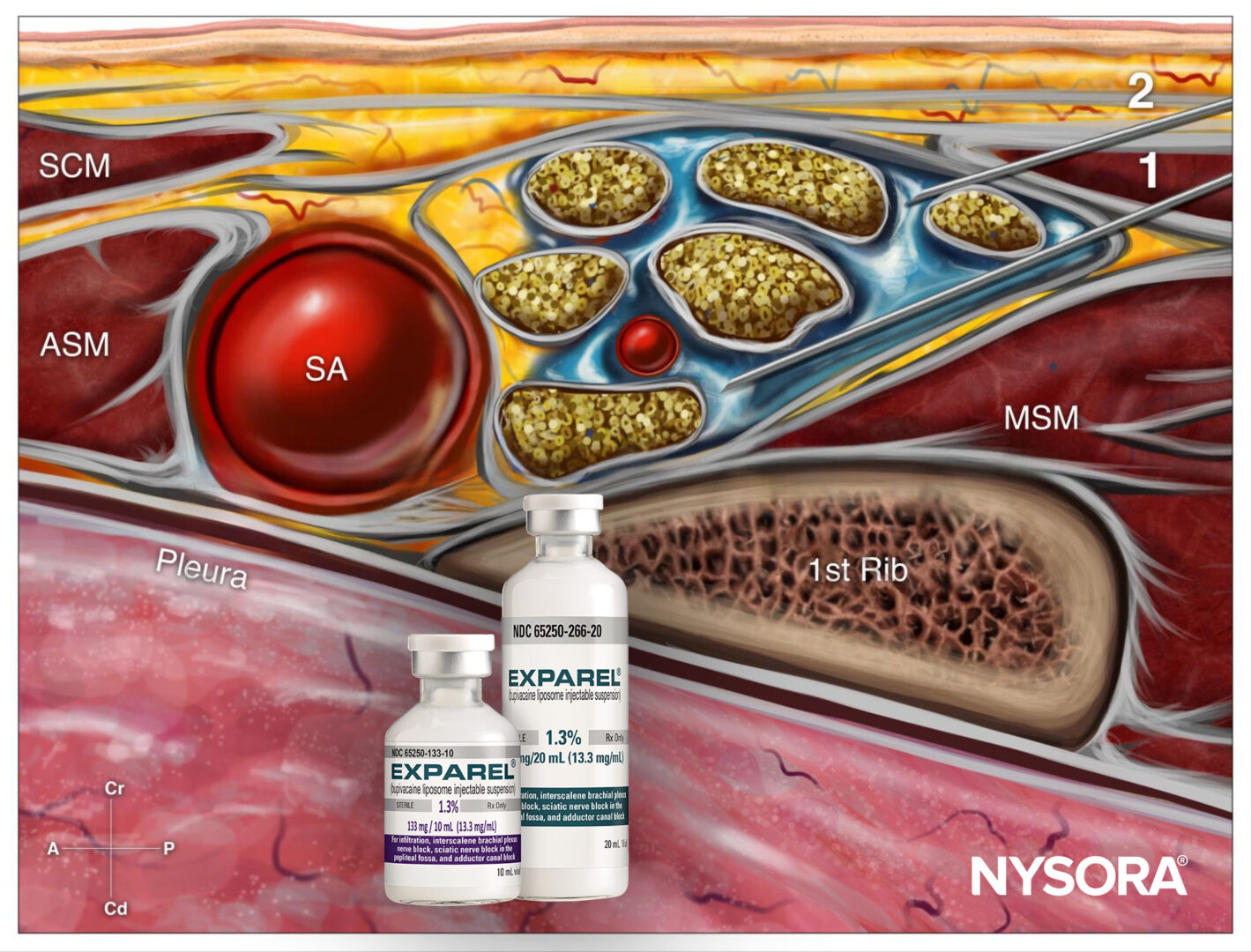
- US-TAP: Administered preoperatively using the posterior approach, with 20 mL of 0.2% ropivacaine per side injected under ultrasound guidance.
- L-TAP: Delivered intraoperatively via a laparoscopic dual subcostal approach, with 40 mL of 0.2% ropivacaine bilaterally.
- Blinding was maintained for clinicians and patients to ensure objective outcome assessment.
Key findings
The results highlighted nuanced differences between block techniques and placebo:
- Morphine use:
-
- L-TAP demonstrated superiority over placebo, reducing morphine use by 5.9 mg on average (p = 0.01).
- US-TAP did not differ significantly from placebo (- 1.4 mg; p = 0.55).
- L-TAP was non-inferior to US-TAP, with a 4.5 mg reduction (CI: – 10.0 to 1.1).
- Quality of recovery: No significant differences were observed in patient-reported recovery scores between groups.
- Secondary outcomes: Postoperative nausea and vomiting rates, mobilization ability, and postanesthesia care unit (PACU) length of stay were similar across all groups.
Conclusion
The L-TAP block demonstrated modest benefits, outperforming placebo and proving non-inferior to US-TAP in reducing morphine consumption within the first 24 hours. However, the observed reduction did not meet the predefined clinically meaningful threshold of 10 mg. US-TAP offered no significant advantage over placebo. These findings suggest that while L-TAP provides some analgesic benefit, neither block type should be standard for minimally invasive colon surgeries under ERAS protocols.
Future research
Future studies should explore the role of TAP blocks as rescue analgesics or in procedures with higher postoperative pain levels. Investigating optimal block timing, techniques, and local anesthetic volumes could further refine their utility.
For more detailed information, refer to the full article in RAPM.
Salmonsen CB, Lange KHW, Kleif J, et al. Transversus abdominis plane block in minimally invasive colon surgery: a multicenter three-arm randomized controlled superiority and non-inferiority clinical trial. Reg Anesth Pain Med. Published online November 14, 2024.
Download the Nerve Blocks App HERE for in-depth insights on the transversus abdominis plane block. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks!