Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About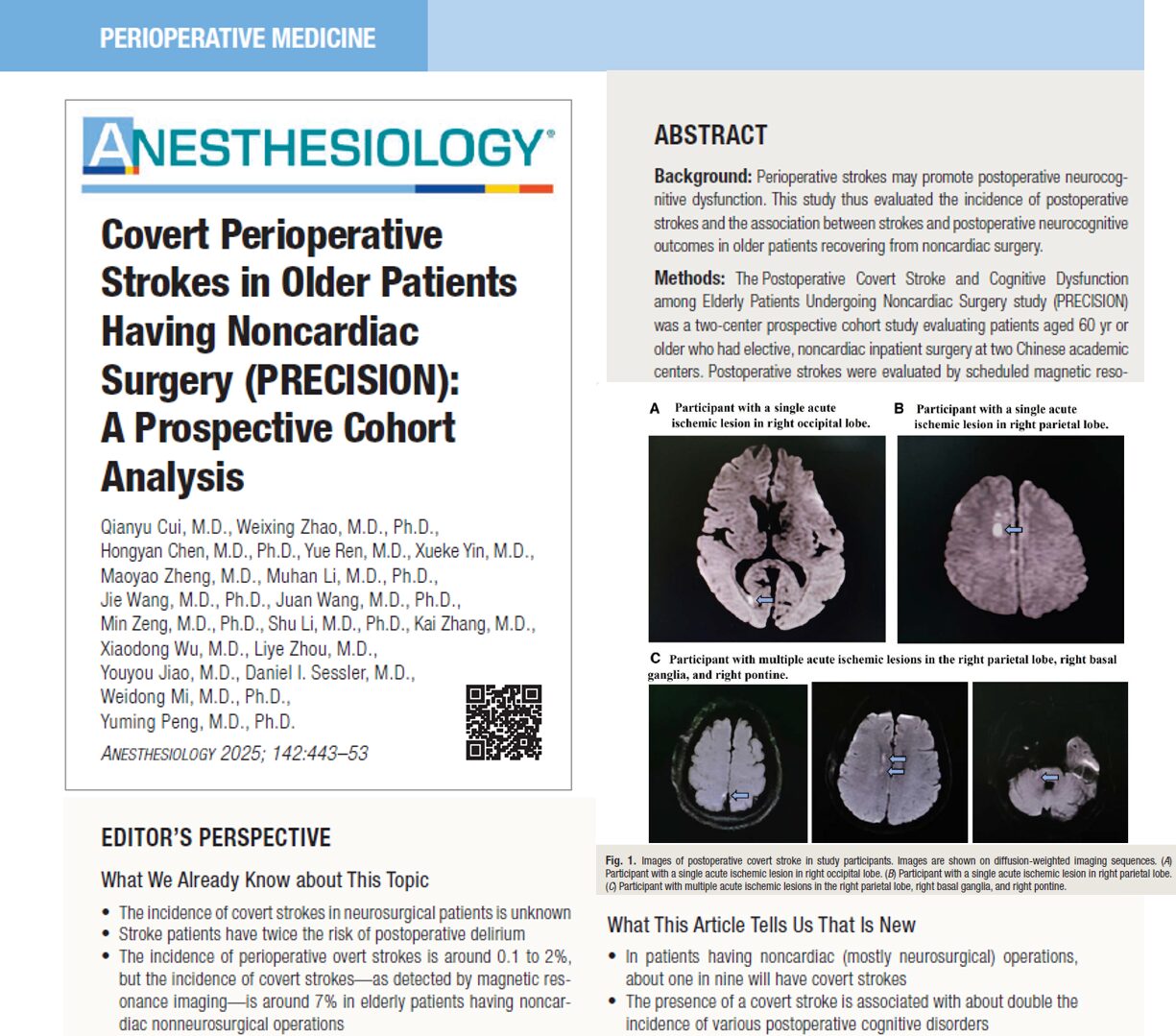



A study published in Anesthesiology (March 2025) reveals that covert strokes—small, symptom-free brain infarcts—occur far more often than expected in elderly patients after noncardiac surgery, especially neurosurgery.
Key takeaways
- Incidence: 11.9% of patients aged 60+ had covert strokes post-surgery.
- No overt strokes: None showed obvious stroke symptoms.
- Consequences:
- Delirium: 23% of patients with covert strokes experienced delirium vs. 11% without.
- Long-term cognitive decline: Risk doubled one year after surgery.
- High-risk group: Neurosurgical patients had the highest stroke rate (16.3%).
What are covert strokes?
- Definition: Brain infarcts visible on MRI, but with no outward neurological signs.
- Significance: Linked to future strokes, cognitive decline, and mortality.
Study Highlights (PRECISION Study)
- Participants: 934 patients, age ≥60, noncardiac surgeries (mostly brain tumor resections).
- Methods:
- MRIs within 7 days post-surgery.
- Cognitive tests pre-surgery, and at 3 months & 1 year.
- Monitored for postoperative delirium.
Primary & secondary outcomes
Primary outcome:
- Cumulative Incidence of Covert Stroke: 111 out of 934 (11.9%).
Secondary outcomes:
- Postoperative Delirium: 12.5% of patients.
- Neurocognitive Decline:
- 3 months: 19.7%.
- 1 year: 18.8%.
- Association:
- Covert stroke → 2.18x increased odds of delirium.
- Covert stroke → 2.33x increased odds of long-term cognitive decline.
Noteworthy Observations
- Lesion characteristics:
- Median diameter: 7 mm.
- Median volume: 185 mm³.
- 77% of neurosurgical patients had multiple acute infarcts.
- Predominant locations: Frontal lobe (60%), basal ganglia, parietal lobe.
- Neurosurgical dominance:
- 66% of surgeries were craniotomies for tumor resections.
- ICU admission impact:
- No significant difference in delirium incidence between ICU and non-ICU patients.
Practical Recommendations for Clinicians
- Preoperative risk stratification:
- Assess age, frailty, ASA classification, stroke history.
- Postoperative monitoring:
- Implement routine MRI screening for high-risk patients.
- Cognitive assessment protocols:
- Utilize validated tools (MMSE, MoCA) both pre- and postoperatively.
- Consider steroid use:
- Evaluate benefits of preoperative corticosteroids, particularly in neurosurgical contexts.
- Multidisciplinary postoperative care:
- Early involvement of neurology and cognitive rehabilitation teams for patients with detected covert strokes.
Conclusion
Covert strokes are common, underdiagnosed, and clinically important. Recognizing and addressing them can improve surgical recovery and brain health in older patients.
Reference: Cui Q, Zhao W, Chen H, et al. Covert Perioperative Strokes in Older Patients Having Noncardiac Surgery (PRECISION): A Prospective Cohort Analysis. Anesthesiology. 2025;142(3):443-453.
For more information on covert strokes, check out Anesthesia Updates on the NYSORA Anesthesia Manual App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.
We asked the Anesthesia Manual App
Should routine MRI screening for covert strokes be considered after major noncardiac surgery in older patients?