Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About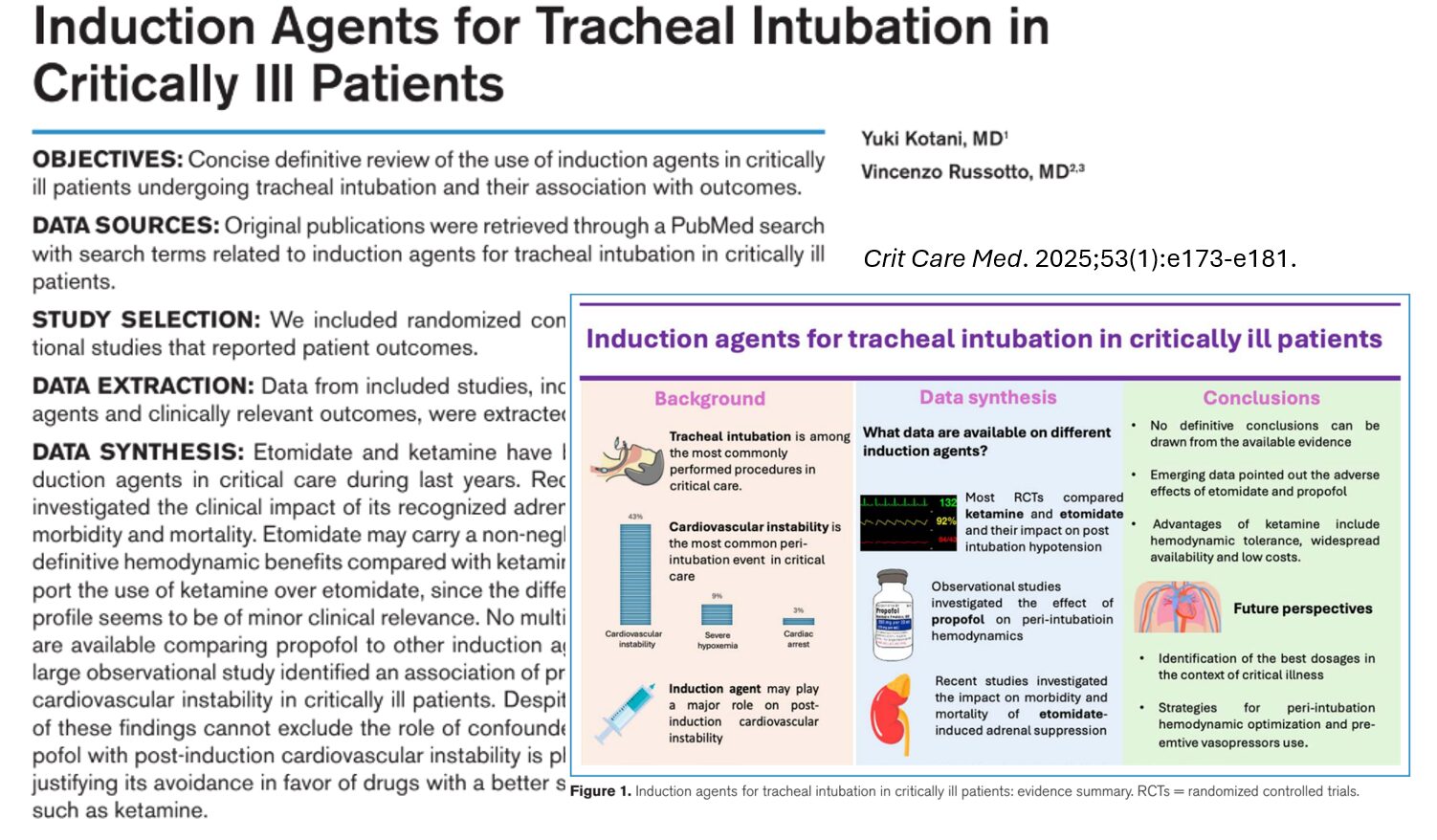





Tracheal intubation is a high-stakes, life-saving procedure commonly performed in intensive care units (ICUs). However, it carries significant risks, especially in critically ill patients who already suffer from physiological derangements like hypoxemia and hypotension. The choice of induction agent can greatly influence patient outcomes.
A recent review by Kotani et al. (Crit Care Med., 2025) examines the pharmacological properties, clinical implications, and comparative safety profiles of commonly used induction agents, including propofol, etomidate, ketamine, midazolam, and thiopental.
Why induction agent choice matters
Critically ill patients are vulnerable to:
- Hypotension (up to 43% post-intubation)
- Hypoxemia (9%)
- Cardiac arrest (3%)
Studies show that post-induction hypotension is linked to higher ICU and 28-day mortality. Therefore, minimizing hemodynamic instability is critical.
Pharmacological profiles and clinical effects
1. Propofol
- Mechanism: GABA receptor agonist
- Effects:
- Rapid sedation
- Myocardial depression and vasodilation
- Risks:
- High rate of cardiovascular instability
- Greater blood pressure drops in elderly or hypovolemic patients
2. Etomidate
- Mechanism: GABA-A receptor agonist
- Effects:
- Hemodynamic stability
- Risks:
- Adrenal suppression (lasting hours to days)
- Potential increased mortality
3. Ketamine
- Mechanism: NMDA receptor antagonist
- Effects:
- Sympathetic stimulation (↑HR, ↑BP)
- Maintains airway reflexes and spontaneous breathing
- Bronchodilation (beneficial in asthma)
- Side effects:
- Hallucinations
- Hypersalivation
4. Midazolam
- Mechanism: GABA receptor agonist
- Effects:
- Sedation and amnesia
- Risks:
- Dose-related hypotension
- Delirium
- Use:
- Often adjunct to other agents
5. Thiopental
- Mechanism: Barbiturate acting on the GABA receptor
- Risks:
- Hypotension, bronchospasm, immunosuppression
- Status:
- Rarely used today
Combination therapy
- Fentanyl: Used for pain, may increase hypotension risk.
- Ketofol (ketamine + propofol):
- Balances hemodynamic effects
- Favorable profile in some studies, but lacks standard dosing protocols.
Emerging evidence and clinical guidelines
Key studies
- INTUBE study: Propofol linked to cardiovascular instability.
- Matchett et al. (Intensive Care Med. 2022): Higher 7-day mortality with etomidate vs. ketamine (23% vs. 15%).
- Meta-analysis: Etomidate is associated with increased mortality risk.
Guidelines
- Difficult Airway Society & SCCM: Prefer ketamine over etomidate.
- SCCM 2023: Etomidate acceptable but not superior to ketamine.
Future directions
Research gaps
- Optimal dosing strategies
- Best practices for vasopressor use
- Efficacy of newer agents like remimazolam
Ongoing trials
- PREVENTION trial: Preemptive vasopressor use
- RSI trials: Long-term outcomes of sedative choice
Conclusion
While no single agent is perfect, ketamine currently stands out as the most suitable induction drug for tracheal intubation in critically ill patients. Propofol and etomidate, while useful in specific contexts, carry risks that may outweigh their benefits. Ongoing research aims to refine these choices further and improve patient outcomes.
Reference: Kotani Y et al. Induction Agents for Tracheal Intubation in Critically Ill Patients. Crit Care Med. 2025;53:e173-e181.
For more information on induction agents, check out Anesthesia Updates on the NYSORA Anesthesia Manual App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.
AI on Call: Case of the week
A 62-year-old man with a history of congestive heart failure and sepsis is in the ICU with worsening respiratory distress and altered mental status. His blood pressure is 88/50 mmHg, his heart rate is 112 bpm, and his oxygen saturation is 85% on a non-rebreather mask. The decision is made to proceed with emergency tracheal intubation.
The team prepares for rapid sequence induction. Which induction agent would you use?