Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Define and classify the different types of psoriasis
- Describe psoriasis triggers
- Anesthetic management of a patient with psoriasis
Definition and mechanisms
- Psoriasis is a chronic skin disorder characterized by an accelerated epidermal turnover and epidermal hyperplasia
- Autoimmune disease resulting from an increased rate of epidermal protein synthesis, rapid epidermal cell growth, shortened epidermal cell cycle, and increase in the proliferative cell population
- Lesions consist of sharply demarcated, loosely adherent, thickened, noncoherent, silver skin scales with increased vascularity → they most commonly appear on the extensor surfaces (i.e., elbows and knees), lumbar-sacral area, and scalp
- Injury to the skin can trigger psoriatic skin changes at that spot (Koebner’s phenomenon)
Classification
- Plaque psoriasis or psoriasis vulgaris
- Most common type (85-90%)
- Causes dry, itchy, raised skin patches (plaques) covered with scales
- Most commonly found on the elbows, knees, scalp, and back
- Nail psoriasis
- Affecting fingernails and toenails
- Causes pitting, abnormal nail growth, and discoloration
- Nails might loosen and separate from the nail bed (onycholysis)
- Guttate psoriasis
- Primarily affects young adults and children
- Triggered by a bacterial infection (e.g., strep throat)
- Marked by small, drop-shaped, scaling spots on the trunk, arms, or legs
- Inverse psoriasis
- Mainly affects the skin folds of the armpits, groin, buttocks, and breasts
- Causes smooth patches of inflamed skin that worsen with friction and sweating
- Fungal infections may trigger this type of psoriasis
- Pustular psoriasis
- Causes clearly defined pus-filled blisters
- Occur in widespread patches or on small areas of the palms or soles
- Erythrodermic psoriasis (erythroderma)
- Least common type
- Widespread inflammation and exfoliation of the skin over most of the body surface (>90% of the body surface area)
- Accompanied by severe dryness, itching, swelling, and pain
- Can develop from any type of psoriasis
Signs and symptoms
- Patchy rash ranging from spots of dandruff-like scaling to major eruptions across the entire body
- Rashes that vary in color (purple with gray scale to pink-red with silver scale)
- Small scaling spots
- Dry, cracked skin that may bleed
- Itching, burning, or soreness
- Cyclic rashes that flare for a few weeks or months and then subside
- Psoriatic lesions become colonized by bacteria (especially Staphylococcus aureus)
- Severe psoriasis may be associated with hyperuricemia, anemia, negative nitrogen balance, iron loss, and hypoalbuminemia
Complications
- Psoriatic arthritis, which resembles seronegative rheumatoid arthritis
- Temporary skin color changes (postinflammatory hypo- or hyperpigmentation) where plaques have healed
- Eye conditions (e.g., conjunctivitis, blepharitis, and uveitis)
- Obesity
- Diabetes type 2
- Hypertension
- Cardiovascular disease
- Other autoimmune diseases (e.g., ulcerative colitis, Crohn’s disease, celiac disease, or multiple sclerosis)
- Increased risk of developing non-melanoma skin cancer
- Mental health conditions (e.g., low self-esteem and depression)
Risk factors
- Genetic (HLA-Cw6)
- Family history
- Smoking
Psoriasis triggers
- Infections (e.g., strep throat or skin infections)
- Weather (cold and dry)
- Injury to the skin (e.g., cut or scrape, bug bite, or severe sunburn)
- Stress
- Smoking and exposure to secondhand smoke
- Obesity
- Heavy alcohol consumption
- Certain medications (e.g., lithium, beta-blockers, calcium channel blockers, antimalarial drugs, NSAIDs)
- Rapid withdrawal of oral or injected corticosteroids
Treatment
- Topical therapy
- Corticosteroids (i.e., hydrocortisone)
- Vitamin D3 analogs (i.e., calcipotriene and calcitriol) to slow skin cell growth
- Retinoids/vitamin A derivatives (i.e., tazarotene)
- Calcineurin inhibitors (i.e., tacrolimus and pimecrolimus) to calm the rash and reduce the scaly buildup
- Salicylic acid to reduce the scaling of scalp psoriasis
- Coal tar to reduce scaling, itching, and inflammation
- Anthralin to slow skin cell growth
- Phototherapy
- Sunlight
- UVB broadband and narrowband
- UVB
- PUVA
- Oral or injected (systemic) medications
- Corticosteroids
- Retinoids/vitamin A derivatives
- Biologics (i.e., apremilast, etanercept, infliximab, adalimumab, etc.) to suppress the immune system
- Methotrexate to decrease the production of skin cells and suppress inflammation
- Cyclosporine to suppress the immune system
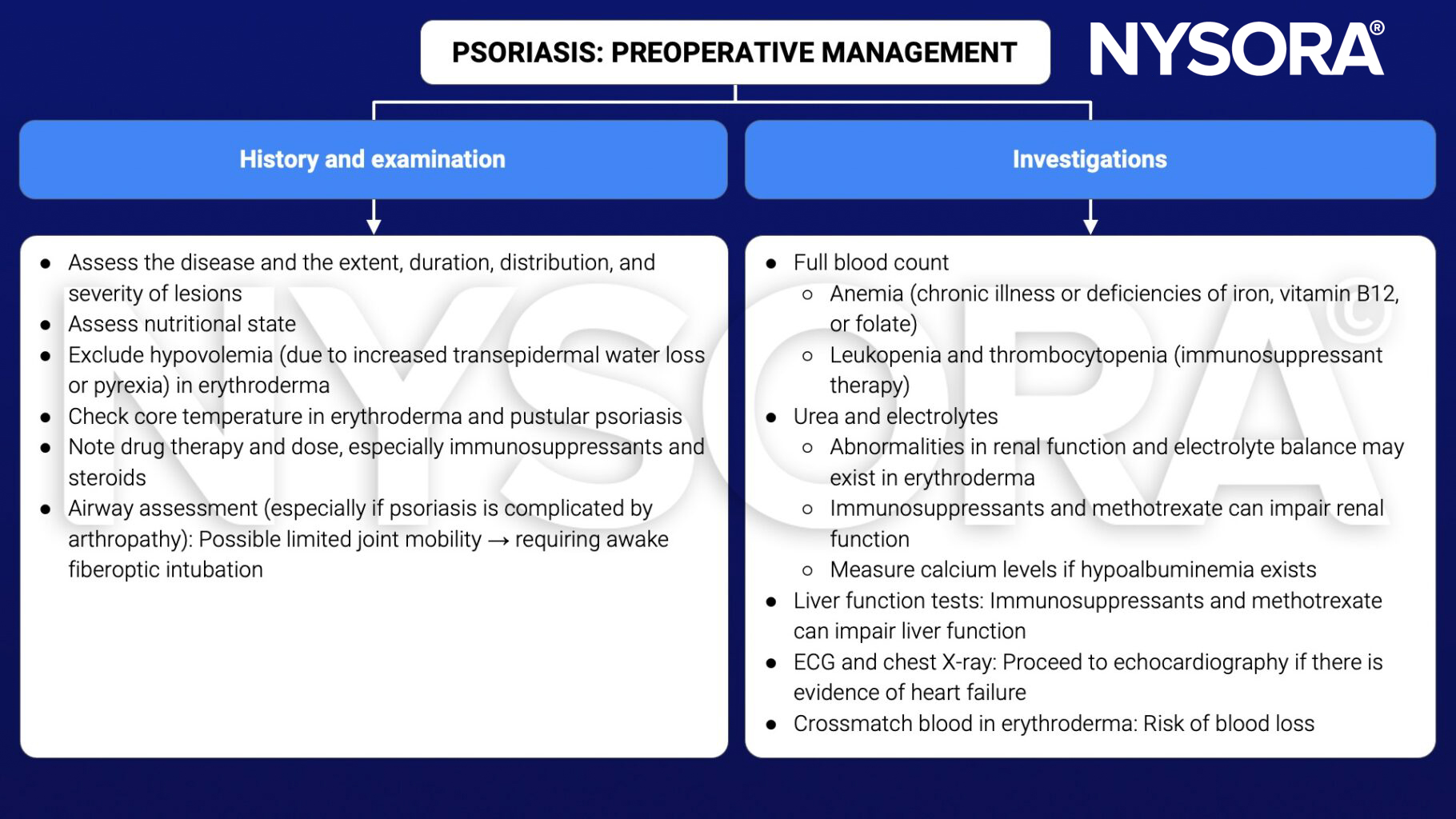
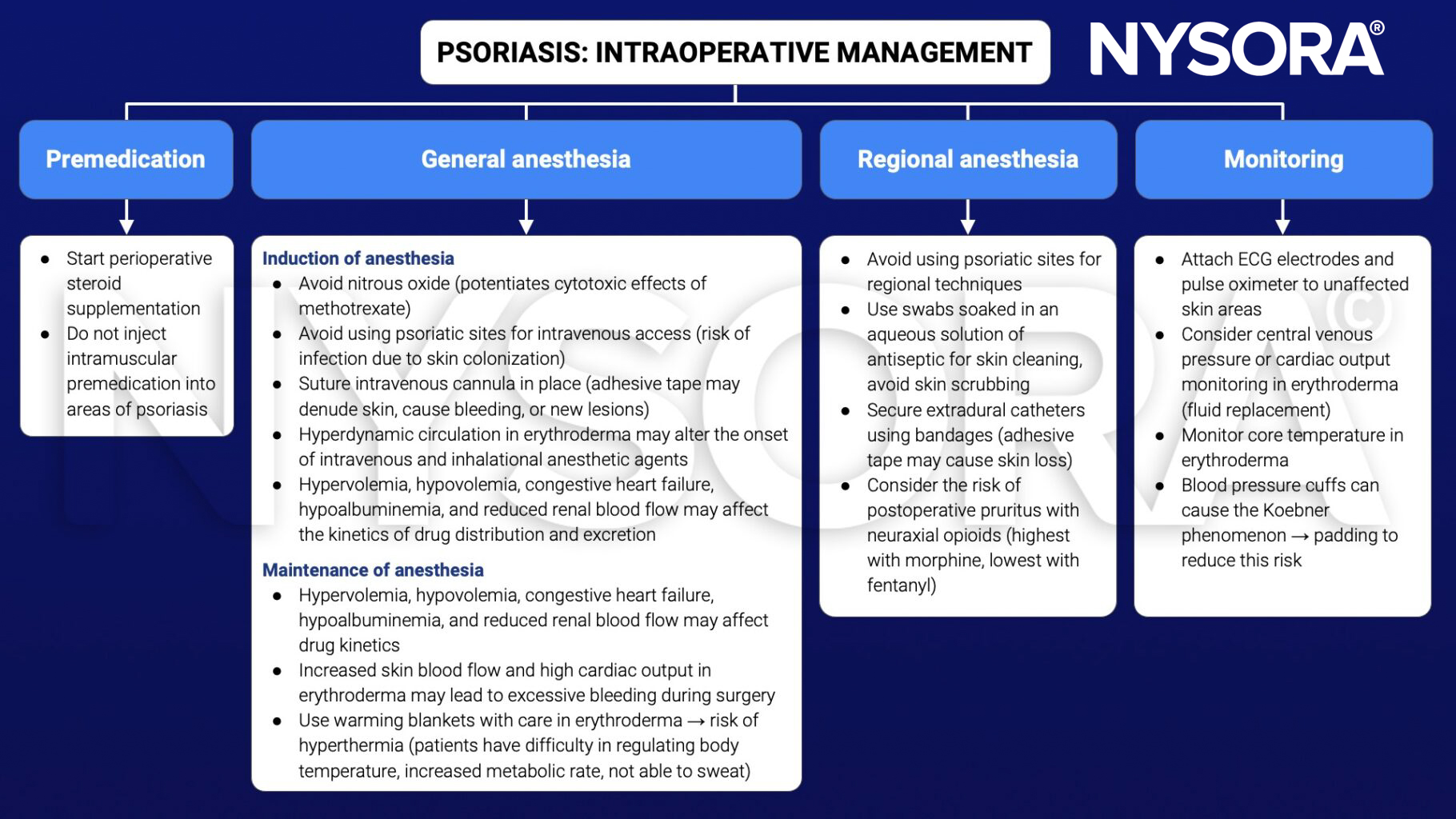
Management
Suggested reading
- Pollard BJ, Kitchen G. Handbook of Clinical Anaesthesia. 4th ed. Taylor & Francis group; 2018. Chapter 9 Connective tissue, Lomas JP.