

Learning objectives
- Describe the major physiological changes during pregnancy
- Describe the anesthetic implications of the physiological changes during pregnancy
Background
- Every major organ system is affected by substantial physiological changes during pregnancy
- Many of these changes significantly affect the pharmacokinetic and pharmacodynamic properties of different therapeutic agents, including anesthetics
- Understanding these changes and their effects is essential to optimize therapy and anesthesia in obstetric patients
Physiological changes
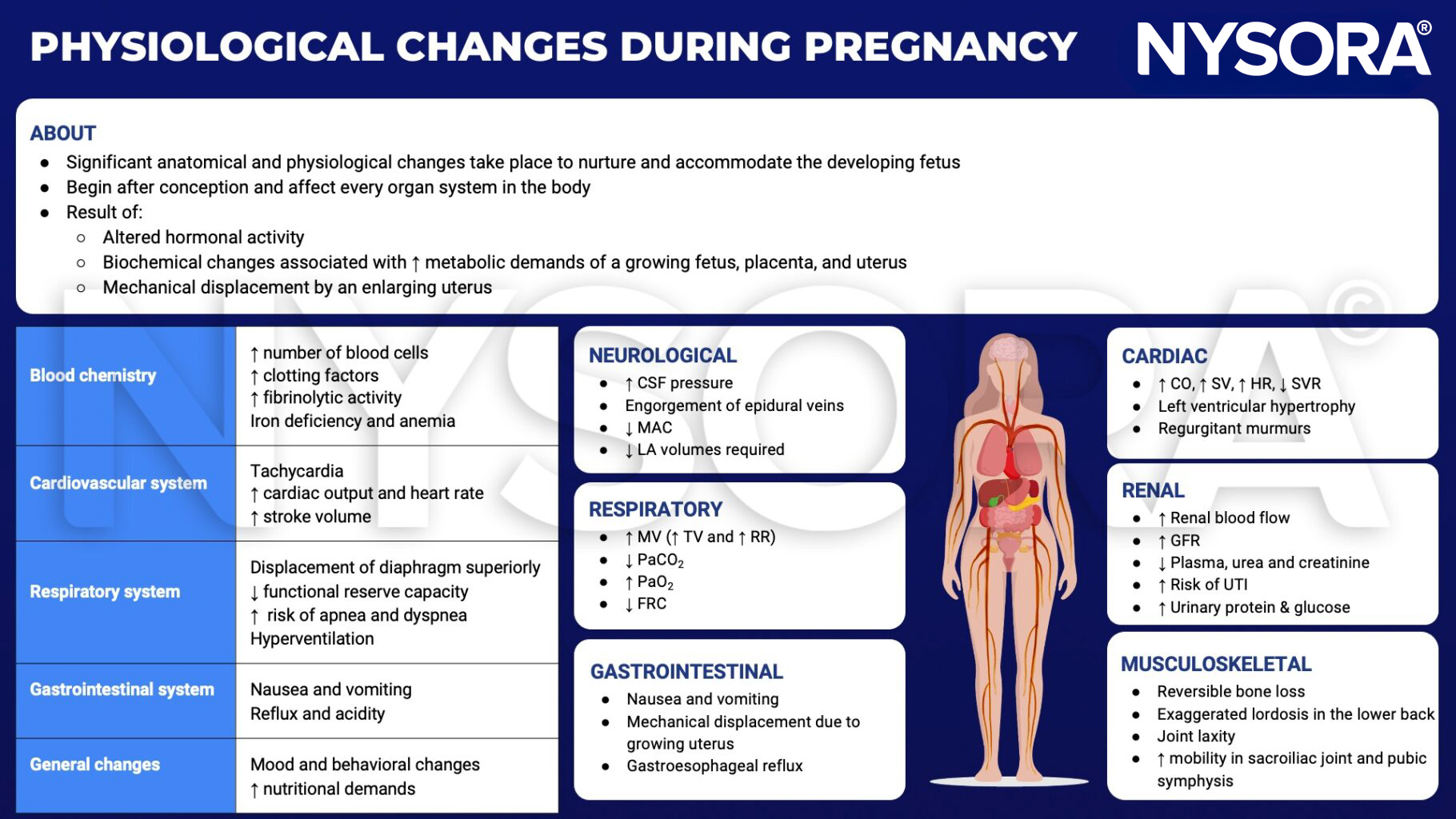
CSF, cerebrospinal fluid; MAC, minimum alveolar concentration; LA, local anesthetic; MV, minute ventilation; TV, tidal volume; RR, respiratory rate; PaCO2, partial pressure of carbon dioxide; PaO2, partial pressure of oxygen; FRC, functional residual capacity; CO, cardiac output; SV, stroke volume; HR, heart rate; SVR, systemic vascular resistance; GFR, glomerular filtration rate; UTI, urinary tract infection
Anesthetic implications
| Cardiovascular | Uterine perfusion not autoregulated |
| Hypotension common under regional and general anesthesia | |
| Supine hypotensive syndrome requires left lateral tilt | |
| Respiratory | Potential hypoxemia in the supine and Trendelenburg positions |
| Breathing more diaphragmatic than thoracic | |
| Difficult laryngoscopy and intubation; bleeding during attempts | |
| Central nervous system | More extensive local anesthetic spread |
| Hematological | Dilutional anemia |
| Thromboembolic complications | |
| Edema, decreased protein binding of drugs | |
| Gastrointestinal | Increased aspiration risk |
| Antacid prophylaxis, RSI after 18 weeks gestation | |
| Renal | Normal urea and creatinine may mask impaired renal function |
| Glycosuria and proteinuria |
Suggested reading
- Costantine M. Physiologic and pharmacokinetic changes in pregnancy. Frontiers in Pharmacology. 2014;5.
- Nejdlova M, Johnson T. Anaesthesia for non-obstetric procedures during pregnancy. Continuing Education in Anaesthesia Critical Care & Pain. 2012;12(4):203-6.
Clinical updates
Rogers et al. (Anesthesiology, 2025) describe pregnancy as a state of progressive insulin resistance, driven by placental hormones, with glucose freely crossing the placenta while insulin does not—making fetal glycemia directly dependent on maternal levels. Insulin resistance peaks in late pregnancy, labor represents a marked metabolic stress state, and insulin sensitivity resets rapidly postpartum in gestational diabetes. These physiologic adaptations explain the increased risk of maternal hyperglycemia, neonatal hypoglycemia, and euglycemic ketoacidosis, with direct implications for obstetric and anesthetic management.
- Read more about this study HERE.











