

Learning objectives
- Anesthetic management of laparoscopic surgery
Definition and mechanisms
- A minimally invasive surgical technique to explore the abdominal and pelvic cavities
- 2-4 small incisions (usually 0.5–1.5 cm) are made to insert surgical instruments and a laparoscope with a camera at the end
- The laparoscope aids in diagnosis or therapeutic interventions
Risks and benefits of laparoscopic surgery
| Benefits | Risks |
|---|---|
| Reduced wound infection Faster recovery Reduced morbidity Reduced pain | Visceral and vascular damage Complications associated with extremes of positioning Acute kidney injury (AKI) Cardiocerebral vascular insufficiency Pulmonary atelectasis Venous air embolism (VAE) 'Well leg compartment syndrome |
List of surgeries performed laparoscopically
- Cyst, fibroid, stone, and polyp removals
- Small tumor removals
- Biopsies
- Tubal ligation and reversal
- Ectopic pregnancy removal
- Endometriosis surgery
- Urethral and vaginal reconstruction surgery
- Orchiopexy (testicle correction surgery)
- Rectopexy (rectal prolapse repair)
- Hernia repair surgery
- Esophageal anti-reflux surgery (fundoplication)
- Gastric bypass surgery
- Cholecystectomy (gallbladder removal) for gallstones
- Appendectomy (appendix removal) for appendicitis
- Colectomy (bowel resection surgery)
- Abdominoperineal resection (rectum removal)
- Cystectomy (bladder removal)
- Prostatectomy (prostate removal)
- Adrenalectomy (adrenal gland removal)
- Nephrectomy (kidney removal)
- Splenectomy (spleen removal)
- Radical nephroureterectomy (for transitional cell cancer)
- Whipple procedure (pancreaticoduodenectomy) for pancreatic cancer
- Gastrectomy (stomach removal)
- Liver resection
Complications
- Occult hemorrhage – may not be visible due to small surgical field
- Vascular or solid organ injury
- Gas embolism
- Subcutaneous emphysema
- Capnothorax: suspect of unexplained ↑ airway P, hypoxemia, & hypercapnia
- Capnomediastinum & capnopericardium
- Complications related to positioning
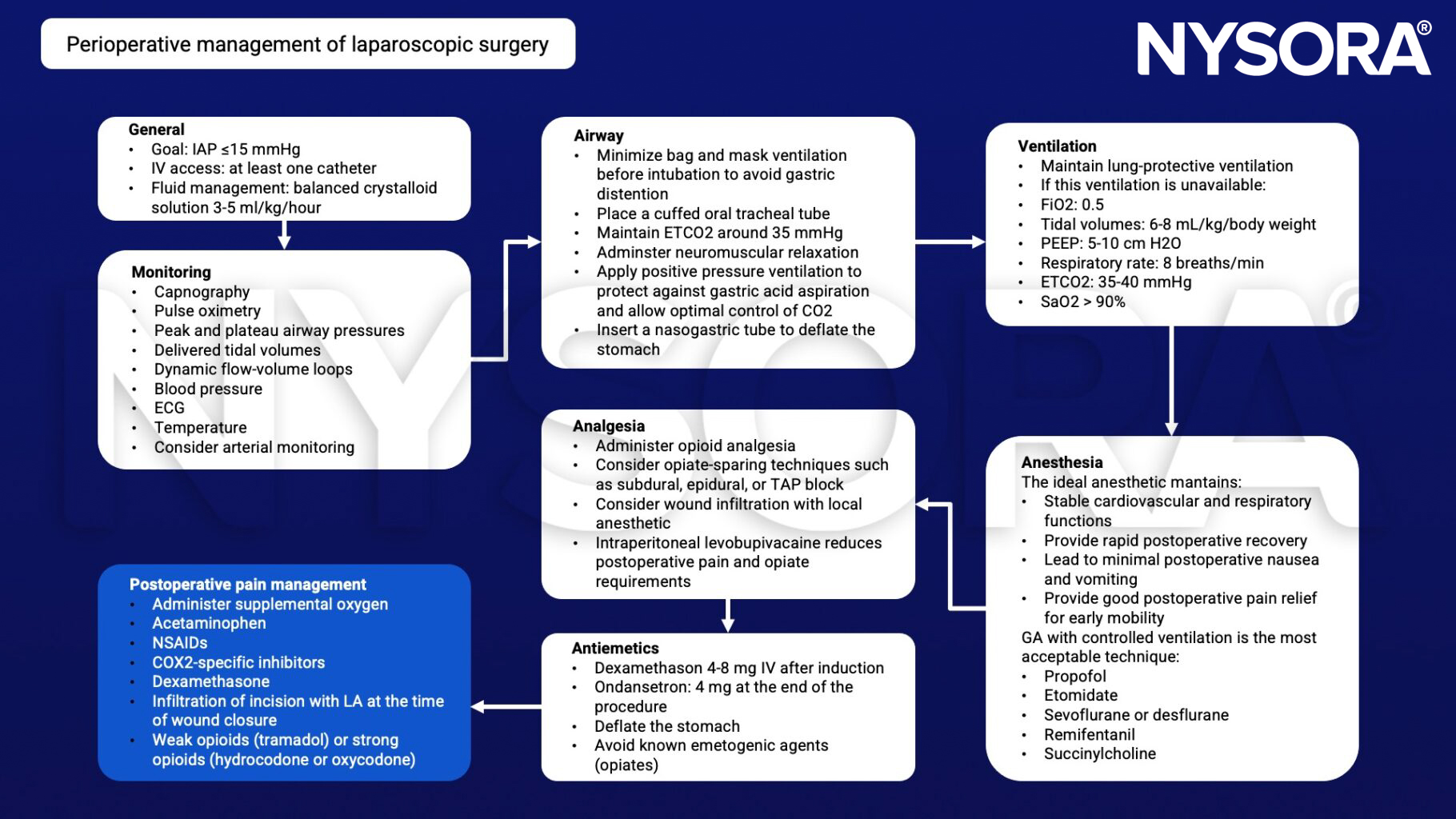
Perioperative management
Suggested reading
- Bajwa SJ, Kulshrestha A. Anaesthesia for laparoscopic surgery: General vs regional anesthesia. J Minim Access Surg. 2016;12(1):4-9.
- Hayden P, Sarah Cowman S. Continuing Education in Anaesthesia Critical Care & Pain, Volume 11, Issue 5, October 2011, Pages 177–180.
Clinical updates
Turunc et al. (Regional Anesthesia & Pain Medicine, 2025) conducted a randomized controlled trial of 60 patients undergoing laparoscopic colorectal surgery and found that bilateral anterior subcostal quadratus lumborum block (QLB) significantly reduced 24-hour opioid consumption (15 mg vs 24.3 mg IV morphine equivalents) and 12-hour consumption (8 mg vs 15.1 mg), prolonged time to first PCA use (45 vs 20 min), and reduced rescue analgesic (7.4% vs 57.1%) and antiemetic use (18.5% vs 71.4%). Sensory spread consistently covered T7-L1 dermatomes (with partial T6 involvement in 63%), and the QLB group demonstrated earlier mobilization (12 vs 17 hours) and shorter hospital stay (5 vs 6 days), with no block-related complications reported.
Lirk et al. (European Journal of Anaesthesiology, 2024) performed a PROSPECT systematic review of 72 RCTs and recommend baseline multimodal analgesia for laparoscopic colorectal surgery consisting of paracetamol plus an NSAID/COX-2 inhibitor for colonic surgery , surgical wound infiltration, and rescue opioids. They do not recommend epidural analgesia, truncal blocks (TAP, QLB, ESPB), deep neuromuscular blockade, intraperitoneal local anesthetic, or specific surgical techniques because of inconsistent or insufficient procedure-specific evidence, and no consensus was reached for intrathecal morphine or intravenous lidocaine (the latter may be considered only when basic analgesia cannot be provided).











