Learning objectives
- Recognize the different classes of cardiomyopathies
- Anesthetic management of patients with cardiomyopathy
Definition & mechanisms
- Cardiomyopathy is myocardial disorder in which the heart muscle is structurally and functionally abnormal
- Can be inherited or acquired
- Can affect all age groups
- Affects the shape, function, and electrical system of the heart.
- Signs and symptoms can usually be managed successfully and patients can have a good life expectancy
Dilated cardiomyopathy
- Dilatation of the left and right ventricles, impaired systolic function
- Major cause of heart failure and arrhythmia in young adults
- Two-thirds of cases are idiopathic
- Possible causes:
- Familial association
- Post-viral infection
- Part of a disease process (ischemic heart disease, hypertension, diabetes, malformation syndrome, alcohol excess, neuromuscular disorder, inborn errors of metabolism, exposure to cardiotoxic agents)
- Asymptomatic in early stages
- Symptoms of heart failure (dyspnea, fatigue, ascites, peripheral edema, arrhythmias)
- Embolic events and sudden death may occur at a later stage
- Diagnosis: Echocardiography, chest radiograph, electrocardiography, blood tests, detailed medical and family history, physical examination
Management
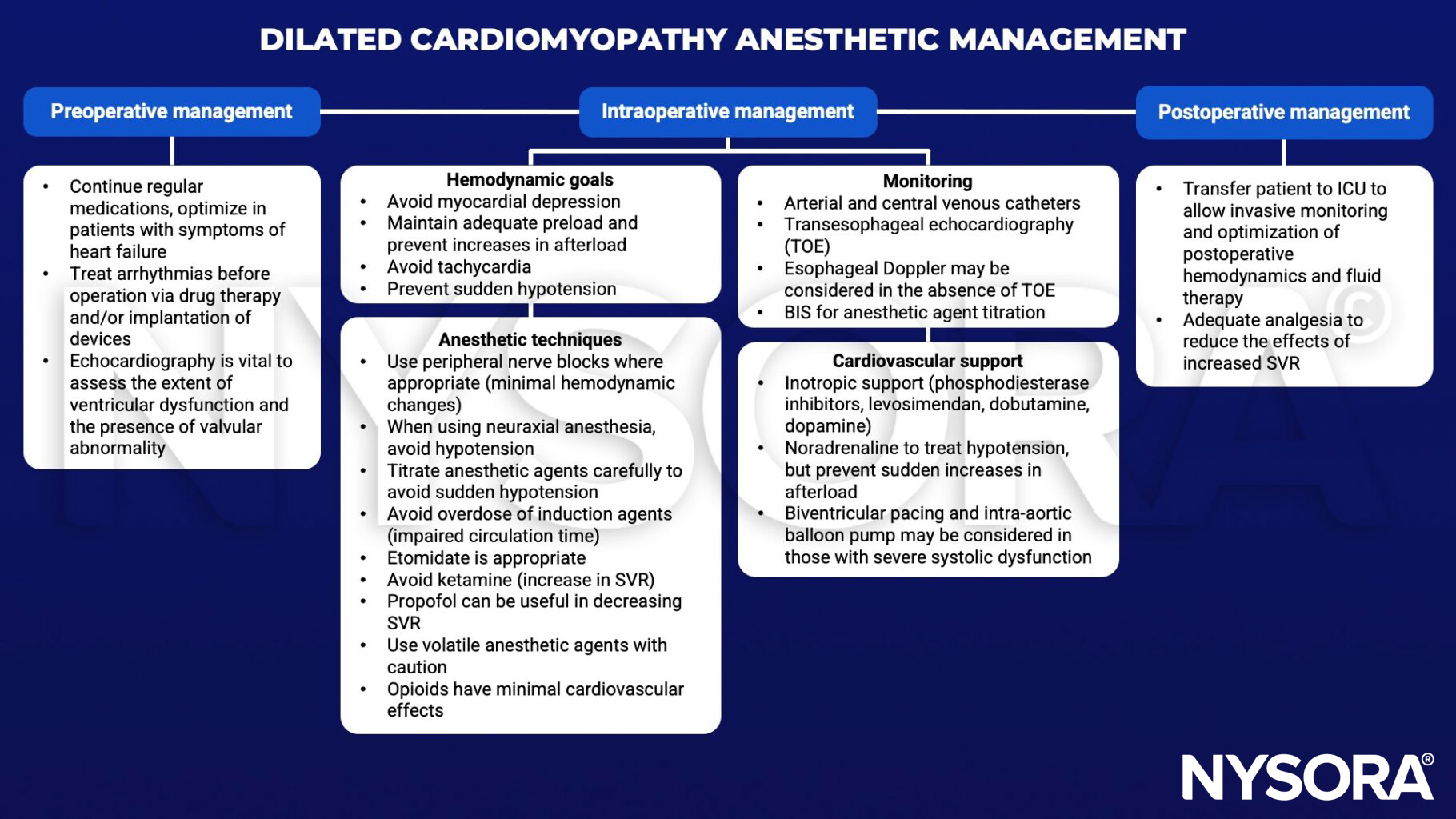
SVR, systemic vascular resistance; BIS, bispectral index; ICU, intensive care unit
Hypertrophic cardiomyopathy
- Hypertrophy of the left ventricle in the absence of other structural or functional abnormalities
- Inherited disease of the myocardium
- Hypertrophy can be asymmetrical, concentric, midventricular, apical, and can also involve the right ventricle
- Diastolic impairment of the left ventricle
- End-stage: Biventricular systolic dysfunction due to myocardial fibrosis
- 70% of cases have obstructive hypertrophy
- Majority of patients is asymptomatic
- Symptoms of angina and heart failure (dyspnea, chest pain, syncope, arrhythmia)
- Severe complications: Angina pectoris, heart failure, sudden death
Management
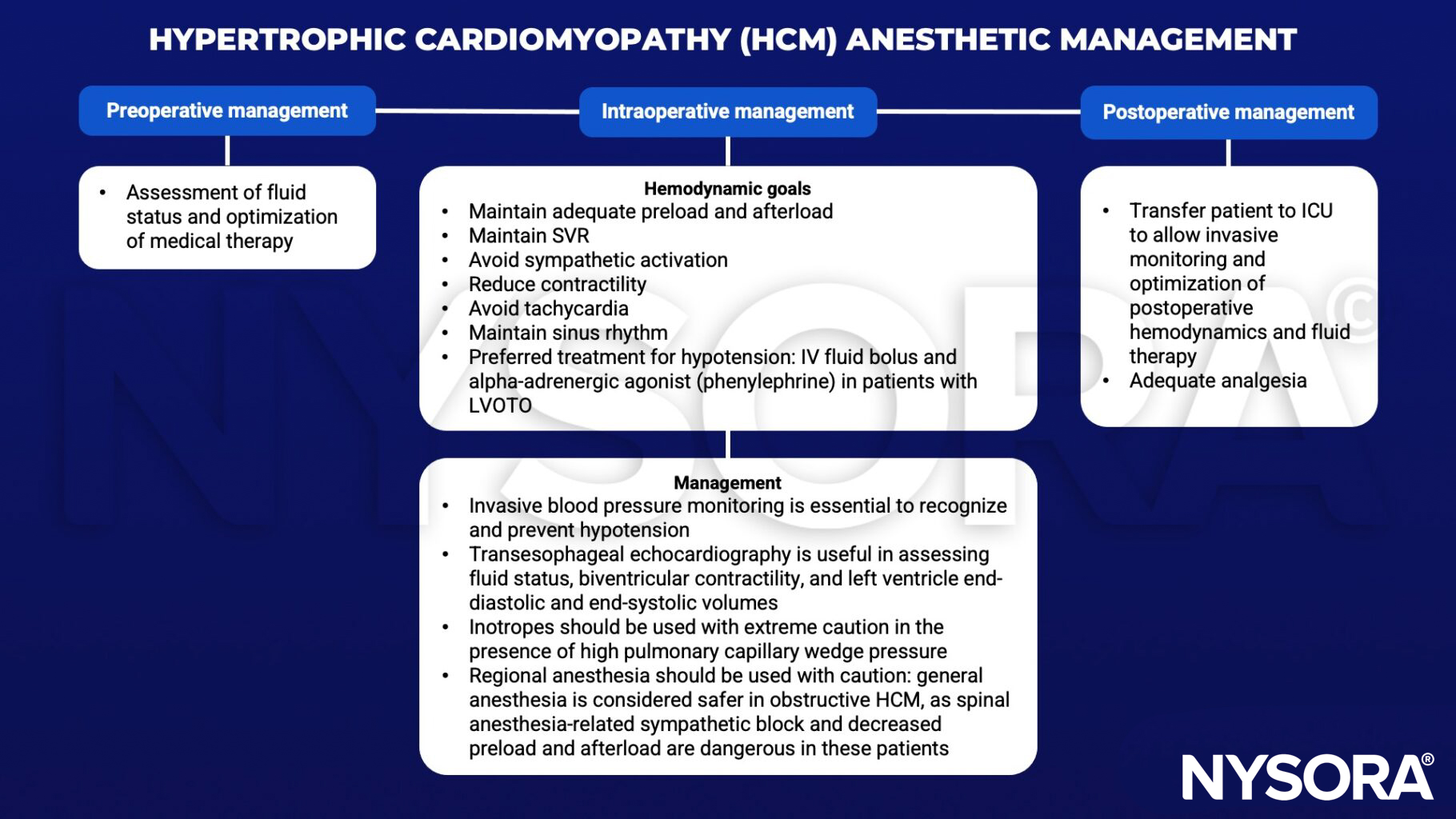
SVR, systemic vascular resistance; LVOTO, left ventricular outflow tract obstruction
Restrictive cardiomyopathy
- Impairment of ventricular diastolic function due to fibrotic or infiltrative changes in the myocardium and/or subendocardium
- Primary or secondary (amyloidosis, sarcoidosis, hemochromatosis, ischemic heart disease, hypertension, valvular disease)
- Symptoms of biventricular failure (dyspnoea, orthopnea, fatigue, palpitation, edema, chest pain)
- On physical examination, patients may have an audible third heart sound, systolic murmur, raised jugular venous pressure, ascites, and peripheral edema
- Diagnosis: Echocardiography, endomyocardial biopsy, computed tomography, cardiac MRI
Management
- General anesthesia causes vasodilation, suppresses the myocardium, and reduces venous return. The latter can be exacerbated by intermittent positive ventilation resulting in cardiac arrest.
- Invasive arterial blood pressure monitoring and transesophageal echocardiography are useful in identifying the causes of cardiovascular instability.
- Hemodynamic goals:
- Maintain adequate preload, SVR, and sinus rhythm
- Use an anesthetic agent with minimal cardiovascular effect (ketamine or etomidate)
Arrhythmogenic right ventricle cardiomyopathy
- Structural abnormalities and cardiac dysfunction of the right ventricle, can also involve left ventricle
- Complex genetic condition
- Other causes: Degenerative disease, infection, inflammation
- Usually starts as a localized disease with regional wall abnormalities
- Development of right bundle branch block followed by right ventricular failure between the fourth and fifth decades of life
- Young patients often present with arrhythmia, syncope, cardiac arrest, or sudden death
- 3 clinical phases:
- Phase 1 (concealed disease): Some structural abnormality in the myocardium, patients can present with sudden cardiac death
- Phase 2 (overt disease): Established structural abnormality of the myocardium, patients present with arrhythmias and syncope
- Phase 3 (End-stage disease): Severe structural changes
Management
- Arrhythmias of both supraventricular and ventricular may occur at any time
- Avoid hypovolemia, hypercarbia, acidosis and lighter depth of anesthesia
- Amiodarone is the first line of medication to treat rhythm disturbances
- Placement of implantable cardioverter defibrillator is beneficial
Suggested reading
- Ibrahim IR, Sharma V. Cardiomyopathy and anaesthesia. BJA Education. 2017;17(11):363-9.
Clinical updates
Smith and Feinglass (Journal of Clinical Anesthesia, 2024) provide a perioperative-focused review of ATTR and AL cardiac amyloidosis, emphasizing that patients are preload-dependent with profound diastolic dysfunction, autonomic instability, and high arrhythmic risk, making induction the most hemodynamically vulnerable phase and often warranting arterial line placement before induction. They highlight diagnostic clues such as low-voltage ECG despite increased wall thickness, apical sparing on strain imaging, and common extracardiac signs (carpal tunnel syndrome, spinal stenosis, macroglossia), and caution against beta-blockers, non-dihydropyridine calcium channel blockers, and digoxin due to conduction disease and toxicity risk, while noting limited evidence to guide neuraxial or regional techniques.
Eerdekens et al. (Current Opinion in Anesthesiology, 2023) review peripartum cardiomyopathy (PPCM) as pregnancy-associated heart failure with reduced ejection fraction, emphasizing its variable global incidence and the potential for significant maternal morbidity, while noting that many patients experience meaningful ventricular recovery within months. They highlight key anesthetic principles: favor vaginal delivery with carefully titrated neuraxial analgesia in stable patients; avoid increases in afterload, preload, and bradycardia; use cautious vasopressor selection in severe LV dysfunction; restrict fluids; and escalate to invasive monitoring or temporary mechanical circulatory support when instability occurs, within a multidisciplinary expert-center framework.
Chapman et al. (BJA Education, 2023) review peripartum cardiomyopathy (PPCM) as an idiopathic LV systolic dysfunction (LVEF <45%) presenting in late pregnancy or early postpartum, with rising incidence and strong associations with African ethnicity, hypertensive disorders, and genetic susceptibility overlapping dilated cardiomyopathy. They emphasise BNP/NT-proBNP to help exclude heart failure, TTE for diagnosis and prognostication (poor outcomes with LVEF <30%, LV dilatation, RV dysfunction), guideline-directed HF therapy compatible with pregnancy (β-blockers, diuretics, hydralazine/nitrates; avoid ACEi/ARB until postpartum), consideration of bromocriptine with anticoagulation, and early MCS/ECMO in refractory shock. For delivery, they recommend multidisciplinary care, vaginal birth with early neuraxial analgesia, invasive monitoring, and cautious vasopressor use, avoidance of rapid oxytocin boluses and carboprost where possible, and careful postpartum preload management to prevent acute decompensation.