Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Recognize sings & symptoms of BrS
- Diagnose BrS
- Manage patients with BrS
Definition & mechanisms
- Brugada syndrome (BrS) is an abnormality of cardiac ion channels that increases the risk of ventricular fibrillation and sudden cardiac death
- Linked to 19 genetic mutations that encode for sodium, calcium, or potassium channels and result in either increase or decrease in their activity
- In up to 80% of patients, no causative genetic mutation can be found
- Thought to be responsible for up to 40% of sudden cardiac death cases in a structurally normal heart
Signs & symptoms
- Palpitations
- Chest discomfort
- Syncope and nocturnal agonal respiration
- Monomorphic ventricular tachycardia is rare but is more often seen in infants and children
- Events typically occur during sleep with increased vagal tone, with fever, or can be precipitated by drugs, alcohol, and electrolyte disorders
- Between 20 and 30% of patients: supraventricular tachycardias (atrial flutter, atrioventricular nodal re-entry, Wolff-Parkinson-White syndrome), atrial fibrillation is seen most frequently
- In critical care, the most common presentation will be a patient with aborted sudden cardiac death
- Many patients remain asymptomatic
Diagnosis
Diagnosis is based on fulfilling the BrS ECG morphological criteria:
- Type 1: A cove shaped (with T-wave inversion) ST-segment elevation 2 mm in V1 and/or V2 when placed in a standard or superior position, either spontaneously or after Na-channel blocking agent administration (e.g., ajmaline/flecainide)
- Additional ECG morphologies:
- Type 2: Saddleback-shaped (with positive T-wave) ST-segment 1 mm in V1 and/or V2
- Type 3: Saddleback or cove-shaped ST-segment elevation <1 mm in V1 and/or V2
- Neither are diagnostic
- The ECG morphology can change with time and an individual with true BrS can manifest all three different morphologies at different times
- Many conditions can reproduce a type 1 Brugada ECG, differential diagnosis:
- Early repolarisation
- Athlete’s heart
- Acute coronary events
- Pulmonary embolism
- Electrolyte disturbance
- Pericarditis
- Myocarditis
- Dissecting aortic aneurysm
- Arrhythmogenic right ventricular cardiomyopathy
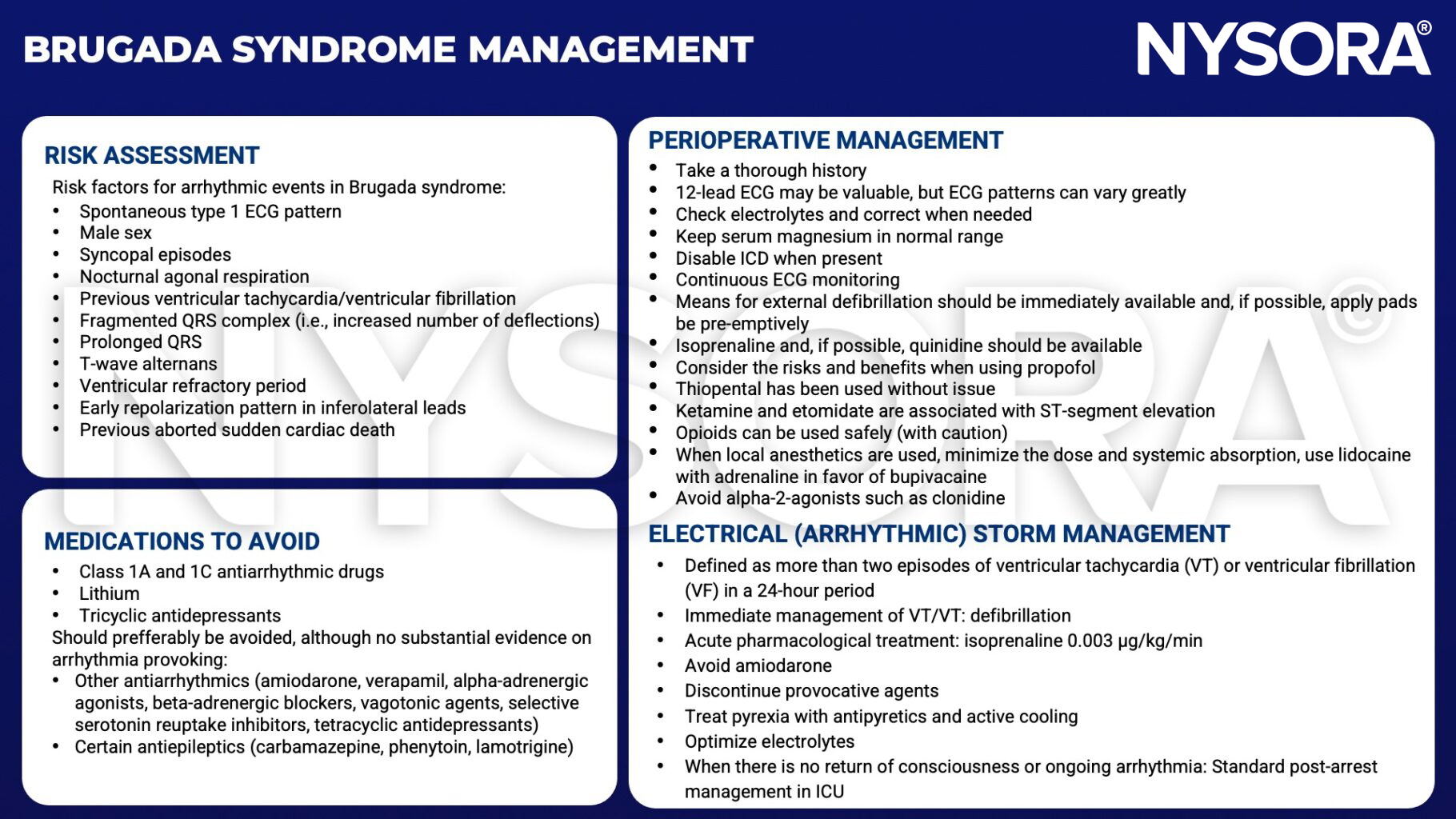
Management
Suggested reading
- Levy D, Bigham C, Tomlinson D. Anaesthesia for patients with hereditary arrhythmias part I: Brugada syndrome. BJA Educ. 2018;18(6):159-165.
Clinical updates
Borrell-Vega et al. (EJA, 2025) report in the BRUGANAES study that across 189 anesthetic procedures in 111 patients with Brugada syndrome over 18 years, malignant intraoperative arrhythmias occurred in only 1% of cases, with no 30-day postoperative arrhythmias or deaths, despite 68% of procedures using traditionally “non-recommended” drugs such as propofol, ketamine, and local anesthetics. Notably, no arrhythmias were observed with neuraxial or peripheral regional techniques, challenging prior assumptions about sodium channel–blocking anesthetics and supporting a more flexible, monitoring-focused perioperative strategy rather than strict drug avoidance in Brugada syndrome patients.
- Read more about this study HERE.