Learning objectives
- Recognize an airway fire
- Management of an airway fire
Definition and mechanisms
- An airway fire is defined as a fire occurring in a patient’s airway
- May or may not include a fire in the attached breathing circuit
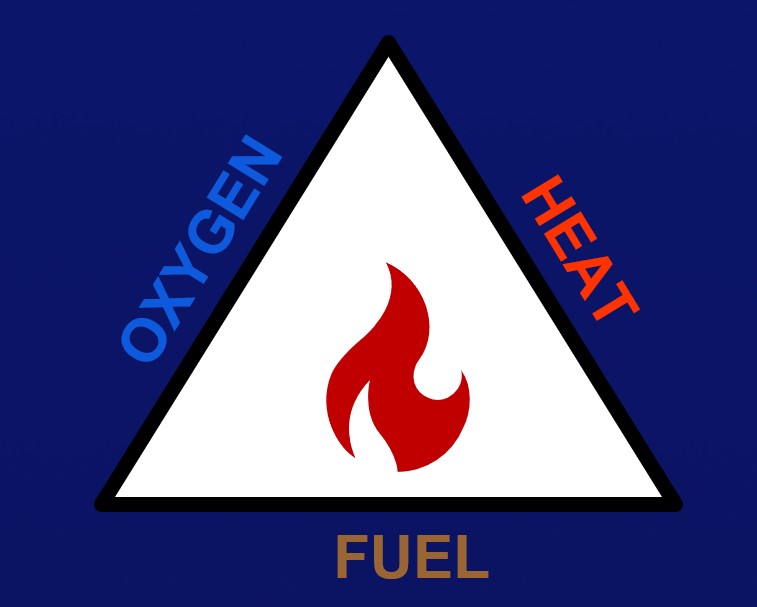
- All airway fires require three components known as the “fire triad”:
- Oxidizers oxygen and nitrous oxide
- Ignition source: electrosurgical devices, lasers, heated probes, burrs and drills, fiberoptic scopes, and defibrillator paddles or pads
- Fuel: tracheal tubes, sponges, drapes, gauzes, alcohol-containing solutions, oxygen masks, nasal cannulae, the patient’s hair, dressings, gowns, gloves, or packaging materials
Prevention
- Determine if the procedure is high-risk
- Agree upon a team plan and team roles for preventing and managing a fire
- Notify the surgeon of the presence of or an increase in an oxidizer-enriched atmosphere
- Before an ignition source is activated:
- Announce the intended use of an ignition source
- Reduce the oxygen concentration to a minimum needed to avoid hypoxia
- Stop the use of nitrous oxide
- Avoid using ignition sources near oxidize-enriched environments
- Configure the drapes to avoid oxidizer pooling or accumulation
- Allow flammable skin-prepping solutions to completely dry
- Sponges and gauzes should be moistened if used near ignition sources
- Airway laser procedures: use laser-resistant cuffed tubes and fill the cuff with saline tinted with methylene blue to identify a cuff puncture by the laser
Management
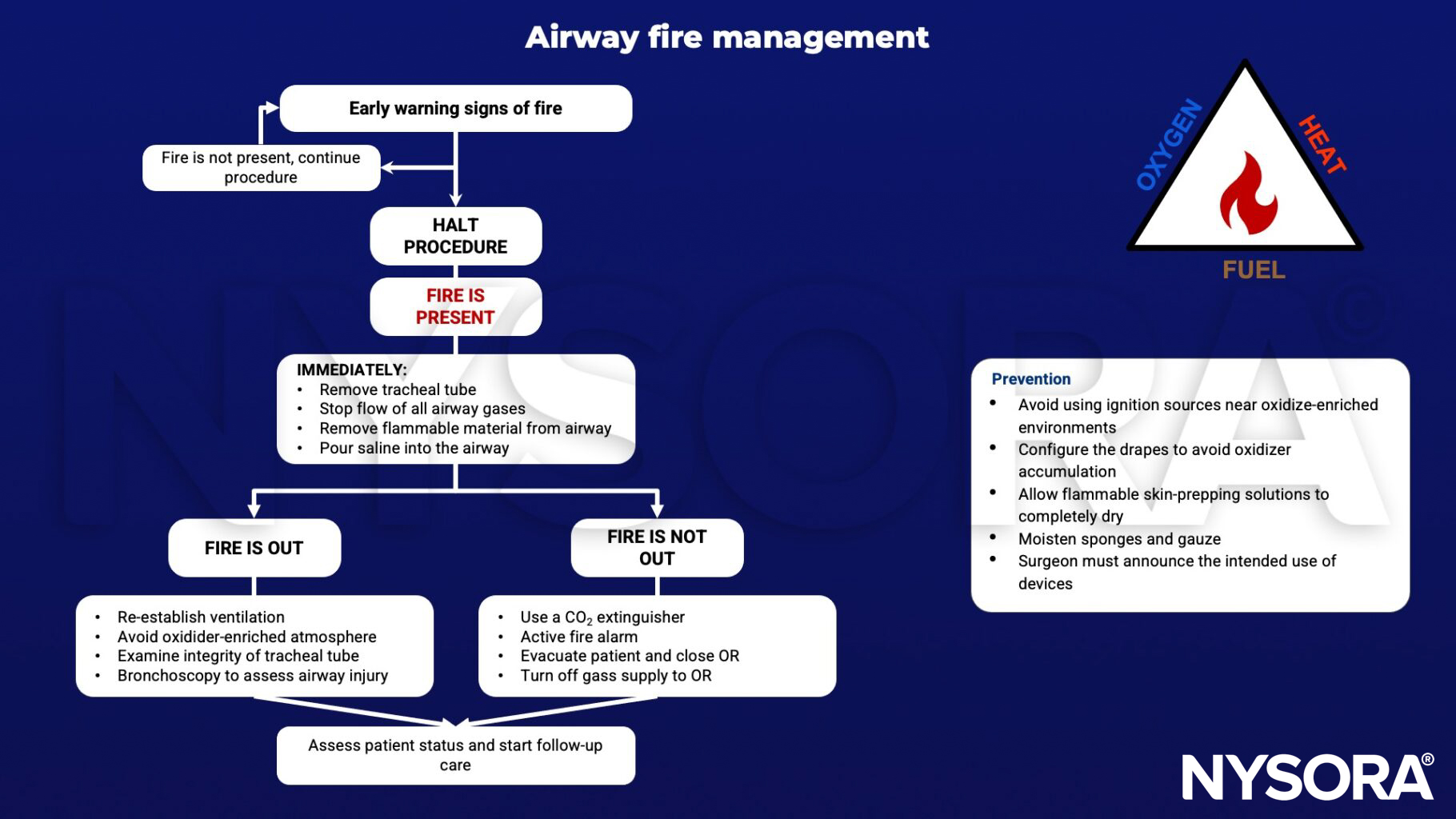
Keep in mind
The following supplies should be immediately available in the operating room:
- Several containers of sterile saline
- A CO2 fire extinguisher
- Replacement tracheal tubes, guides, facemasks
- Rigid laryngoscope blades including a rigid fiberoptic laryngoscope
- Replacement airway breathing circuits and lines
- Replacement drapes, sponges
Suggested reading
- Cowles CE Jr, Culp WC Jr. Prevention of and response to surgical fires. BJA Educ. 2019;19(8):261-266.
- Akhtar N, Ansar F, Baig MS, Abbas A. Airway fires during surgery: Management and prevention. J Anaesthesiol Clin Pharmacol. 2016;Jan-Mar;32(1):109-11.
- Apfelbaum JL, Caplan RA, Barker SJ, et al. Practice advisory for the prevention and management of operating room fires: an updated report by the American Society of Anesthesiologists Task Force on Operating Room Fires. Anesthesiology. 2013;118(2):271-290.
Clinical updates
Lyons et al. (British Journal of Anaesthesia, 2025) raise concern over increasing reports of airway fires associated with high-flow nasal oxygen (HFNO), particularly when FiO₂ is 1.0 and diathermy or laser is used in or near the airway, highlighting multiple published cases and additional MAUDE database reports of burns to the airway, face, and surgical field. They emphasize that open oxygen systems elevate local oxygen concentration, especially under drapes, note that laboratory data support higher fire risk with elevated FiO₂, and recommend avoiding HFNO in the presence of ignition sources except in exceptional circumstances, reducing FiO₂ to the minimum necessary (<0.3 when possible), and ensuring immediate cessation of HFNO if fire occurs.