Etiology
The absence of adequate cerebral perfusion results in cerebral circulatory arrest. It is caused by various conditions of severe brain injury that cause intracranial hypertension, and it accompanies or precedes brain death.
Tip
Cerebral circulatory arrest is sometimes called cerebral tamponade. It can be compared to cardiac tamponade, in which adequate diastolic filling of the heart is not possible due to elevated intrapericardial pressure.
View
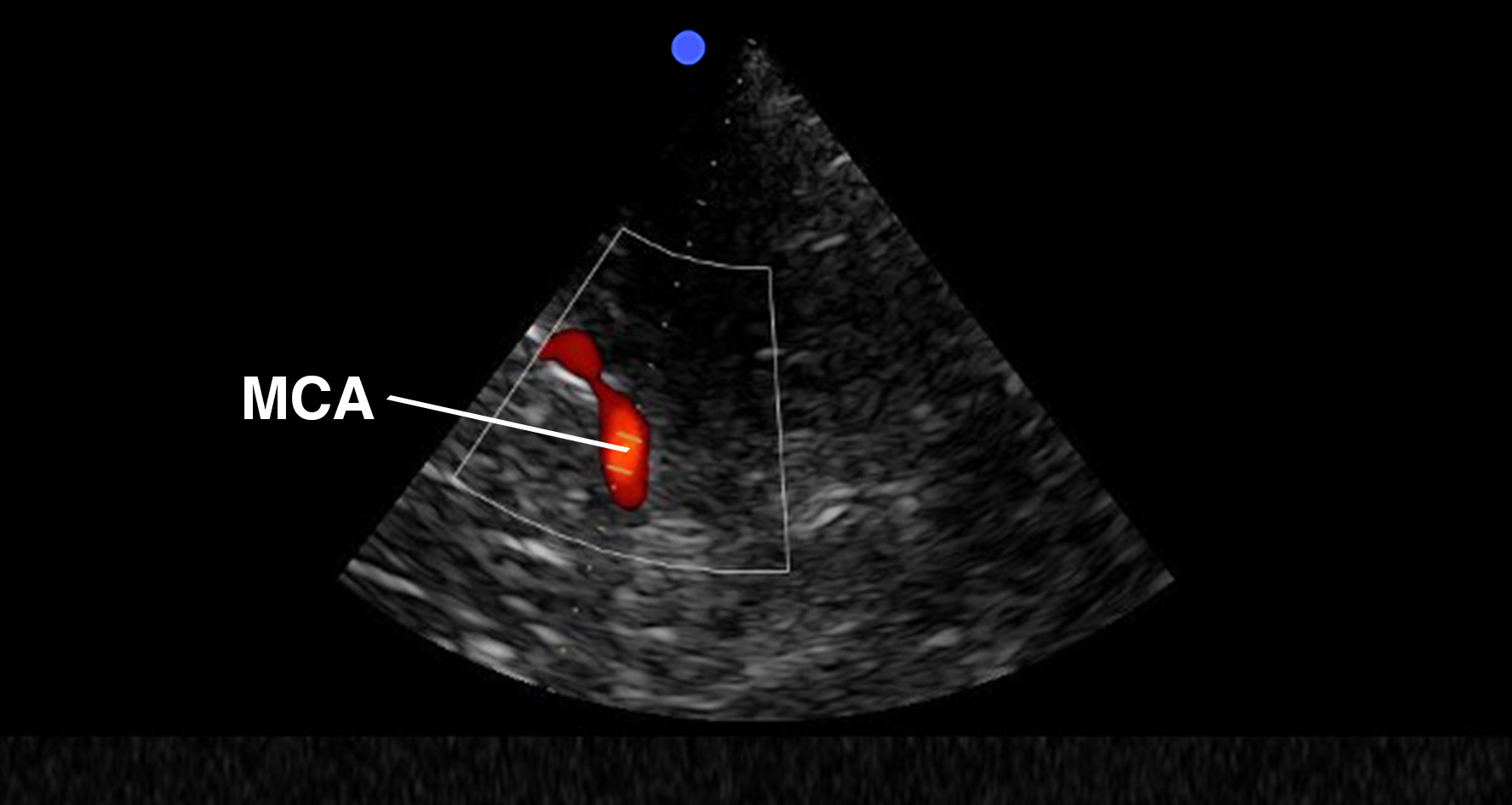
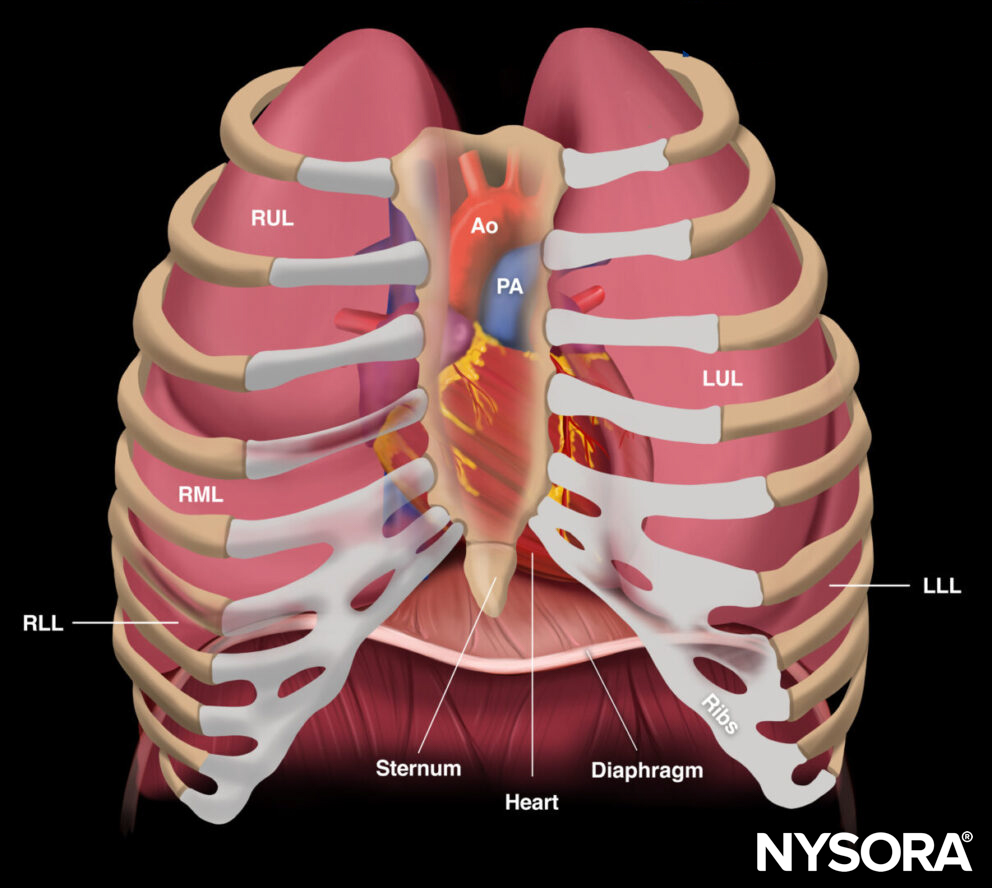
Transducer position for transcranial Doppler examination of cerebral circulatory arrest.
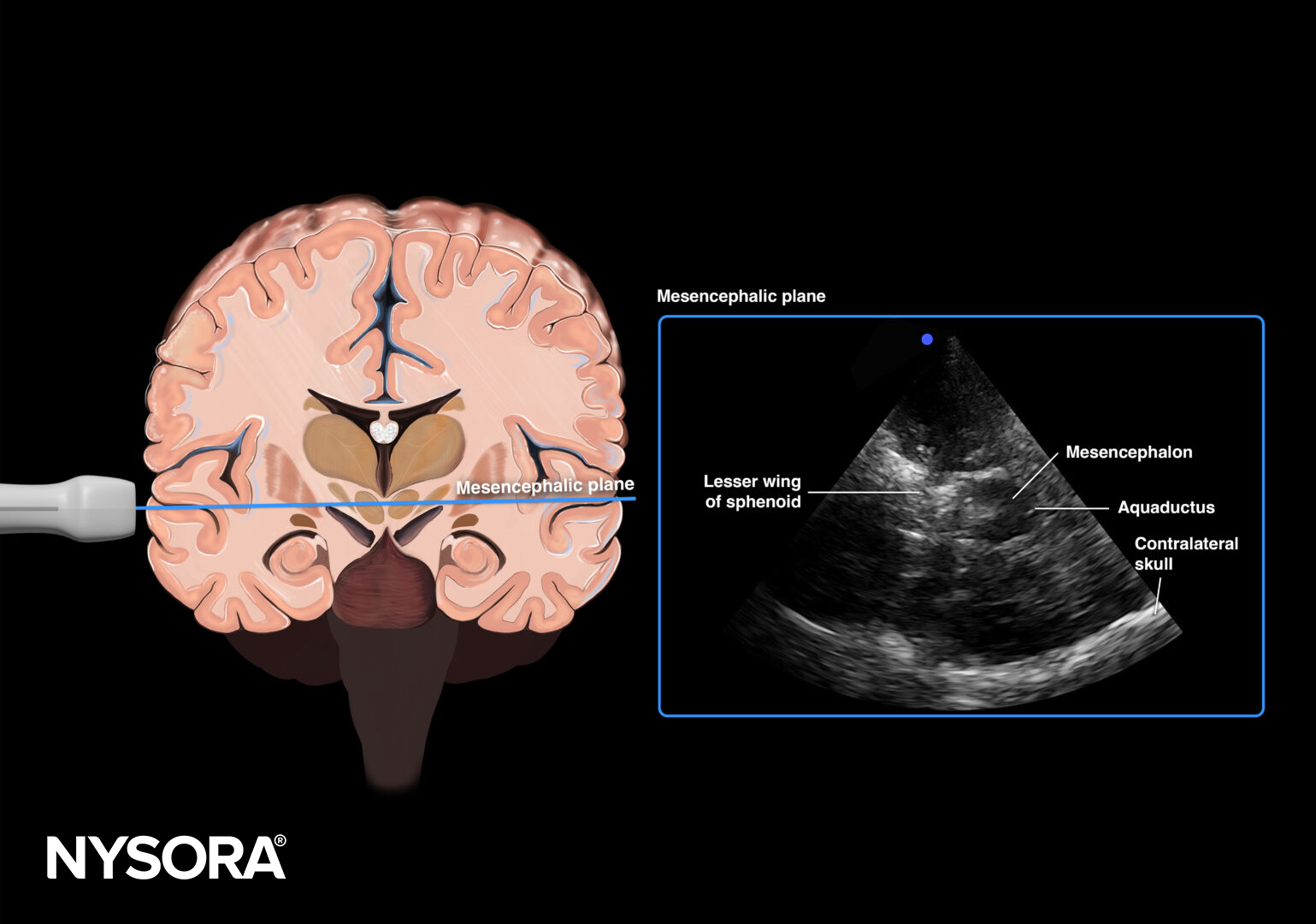
Mesencephalic plane.
Assessment
Use the mesencephalic plane and activate pulsed wave Doppler. Position the Doppler gate on the middle cerebral artery (MCA) and trace the flow velocities.
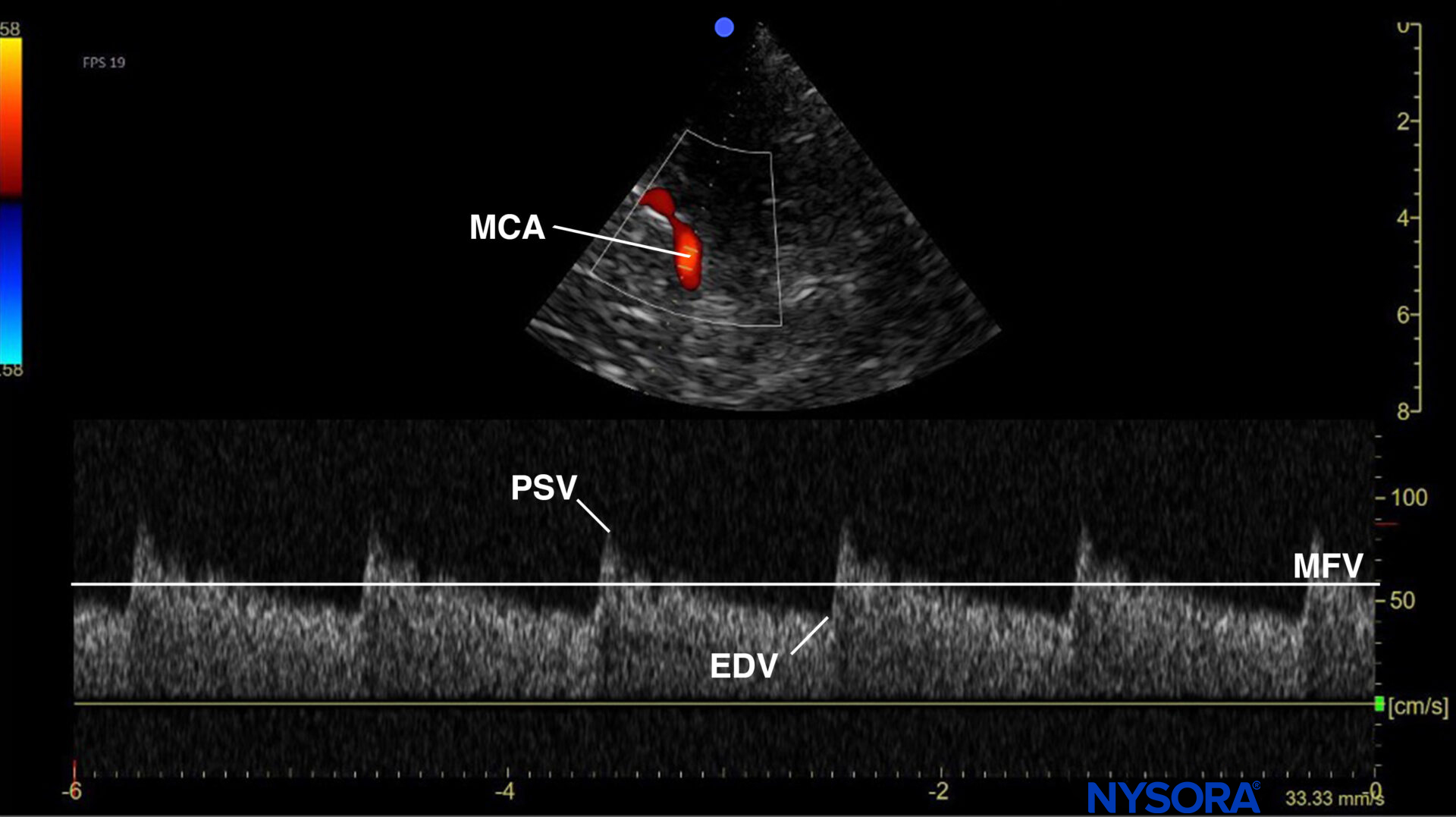
Mesencephalic plane pulsed wave Doppler with the Doppler gate on the middle cerebral artery (MCA). Evaluation of flow velocities in the MCA. PSV, peak systolic velocity; EDV, end-diastolic velocity; MFV, mean flow velocity.
In the presence of elevated intracranial pressure (ICP), different stages of diminished cerebral blood flow can be identified on MCA pulsed wave Doppler.
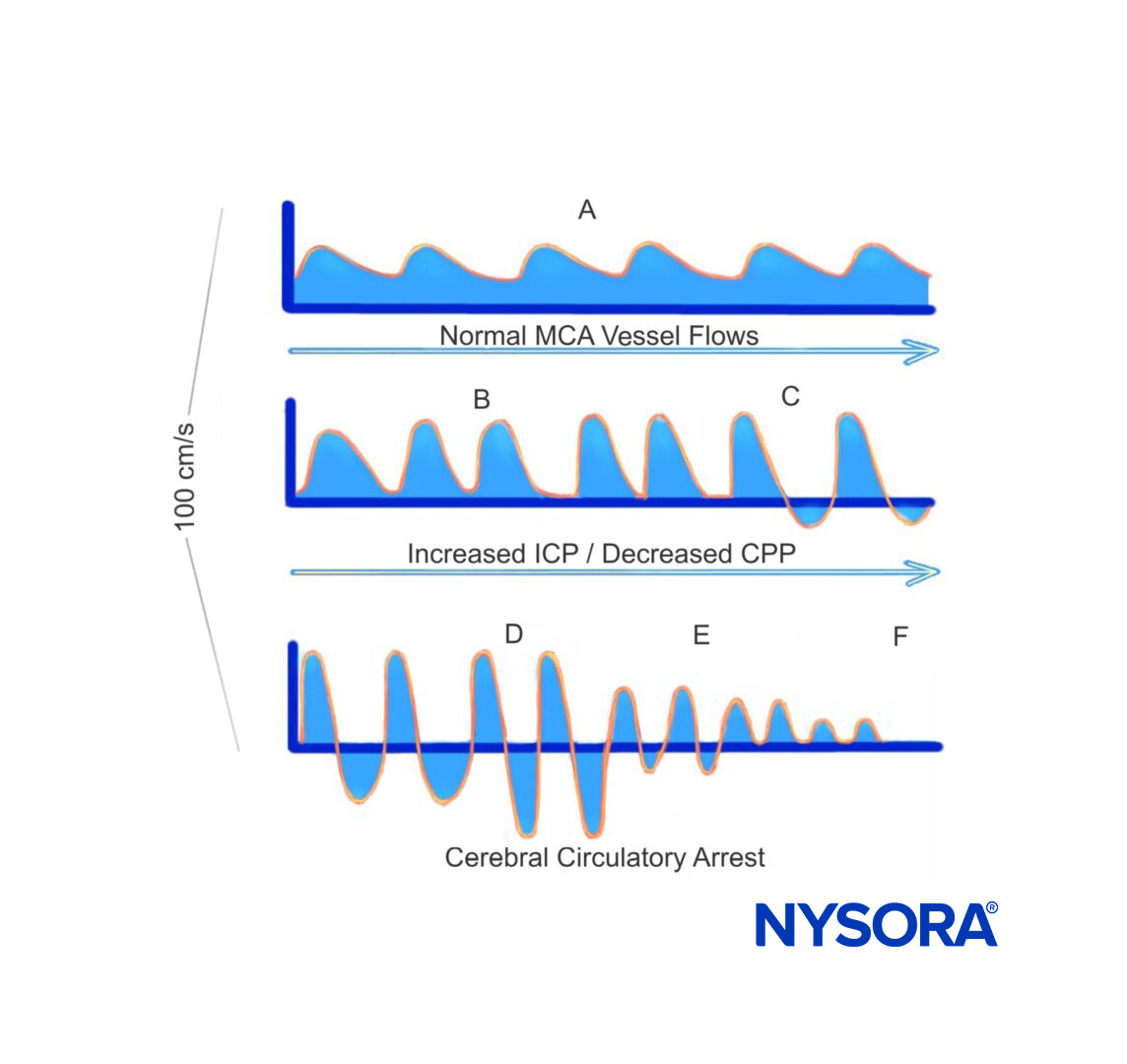
The relationship between middle cerebral artery pulsed wave Doppler and increased intracranial pressure. Adapted from Hassler et al.
Six different phases can be identified in the process of cerebral circulatory arrest, but only the last three phases are considered compatible with cerebral circulatory arrest:
- The systolic and diastolic wave forms are preserved in the early phase.
- Blunting and loss of the diastolic waveform.
- Blood flow reversal during diastole due to high ICP.
- The area under the curve (AUC) during systole equals the AUC during diastole.
- Decrease in systolic flow with eventual no diastolic blood flow. These are also called systolic spikes and usually have flow velocities below 50 cm/s (and duration < 300 ms).
- Absence of cerebral blood flow.
Note
- When the waveform of the AUC above the Y-axis equals the AUC below the Y-axis, blood does not travel to the lungs, and anoxic brain injury will occur.
- In most jurisdictions, brain death is a clinical diagnosis. TCD examination of the MCA flows, however, allows for screening for and better predicting impending brain death.
Clinical updates
- Reynolds et al. (Journal of Neuroimaging, 2025) conducted a scoping review of 181 studies evaluating technical considerations for using transcranial Doppler (TCD) to diagnose cerebral circulatory arrest (CCA) in death by neurologic criteria and found substantial heterogeneity in acquisition parameters, waveform definitions, timing between studies, and required vital sign thresholds. While consistent practices include use of a 2-MHz probe, pulse-wave Doppler with low high-pass filter settings (≤50 Hz), and recognition of oscillating flow or systolic spikes (<200 ms, typically <50–100 cm/s) as patterns consistent with CCA, major gaps remain regarding monitoring duration, vessel requirements, management of skull defects or mechanical circulatory support, and operator credentialing. The authors call for national protocol surveys and Delphi-based expert consensus guidelines to standardize the TCD technique and interpretation for brain death determination.
- Reynolds AS, Suh J, Hasan A, et al. Technical Considerations in the TCD Evaluation of Cerebral Circulatory Arrest in Death by Neurological Criteria. J Neuroimaging. 2025;35(1):e70021.