Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
AboutCannulation of a peripheral vein is an essential skill in medicine and anesthesiology. A peripheral IV access point is required to administer anesthesia, sample blood, infuse fluids and IV medications. Dr. Hadzic will teach a well-known technique for IV placement in difficult patients that is much quicker than using ultrasound.
Dr. Hadzic’s reverse Esmarch technique for difficult IV access
You can do several things to improve the venous flow and enlargement of the veins:
- Apply forced air;
- Warm blankets;
- Warm compresses;
- Or warm IV bags to facilitate venodilatation.
However, these measures take time. Ultrasound can also be used for peripheral access, but ultrasound is not that great a tool for small peripheral veins. Therefore, Dr. Hadzic uses the reverse Esmarch technique to find IV access, draw blood, or cannulate veins even in the most difficult of patients.
Case #1
In this first example, the patient is in the operating room with extremely cold extremities, and it seems impossible to find a distal peripheral vein – a couple of unsuccessful attempts were already made. For this, we use an Esmarch bandage, which is a highly elastic rubber bandage.

- First, we are going to apply a tourniquet and slowly move that tourniquet towards the peripheral aspect of the extremity while consistently squeezing the blood towards the distal extremity.
The Esmarch bandage is applied as a tourniquet while squeezing the blood towards the distal extremity.
- We continue wrapping the extremity while stretching the arm until we get to the distal extremity.
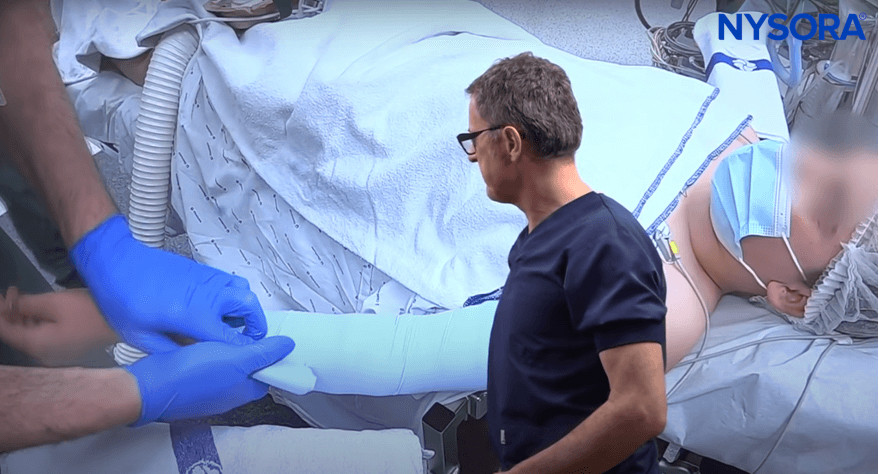
The Esmarch bandage is wrapped around the patient’s arm until the distal extremity is reached.
- As we start assessing the distal peripheral veins, we tap on the skin. Tapping on the skin releases inflammatory mediators and causes venodilatation.
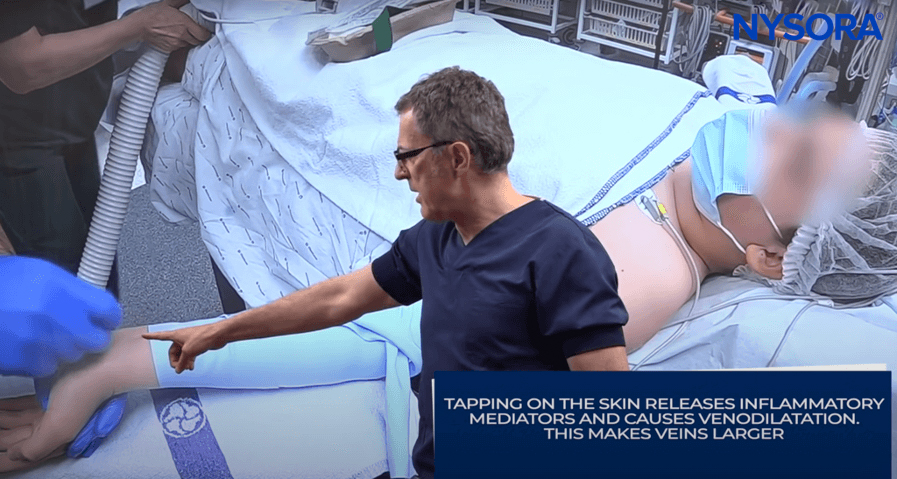
Dr. Hadzic highlights the importance of tapping on the skin.
- Now we can clearly see a good peripheral vein, accessible for cannulation, that was not visible previously.
After applying the reverse Esmarch bandage technique, a peripheral vein becomes accessible for cannulation.
- Another important trick is to slightly bend the needle to lift the needle up and allow a low insertion angle.

Dr. Hadzic demonstrates the bending of the needle and IV catheter placement.
Case #2
We have another example of a patient brought to the operating room with multiple attempts of failed venipuncture.

Dr. Hadzic shows unsuccessful venous punctures.
The IV line was unsuccessful, so we will place the IV line on the other arm. It is important that the arm stays down and is never elevated, as this would drain the blood from the upper extremity. The arm should either hang down or remain horizontal.

Arm in horizontal placement.
The reverse Esmarch bandage is applied to function as a tourniquet. The blood is squeezed distally so that the blood from the deep veins actually pulls down and fills up the small peripheral veins distally. Continue to carefully apply the Esmarch bandage to force blood from deep vessels to the periphery. We “stretch and apply”, moving circularly until we get to the distal extremity.

Esmarch bandage.
We typically use an Esmarch bandage that is 10-15 cm wide.

Esmarch bandage is wrapped around the patient’s arm.
We will continue going on diligently because if you “stretch and apply” with diligence, the Esmarch bandage application is directly proportional to the success you will get with this particular technique.
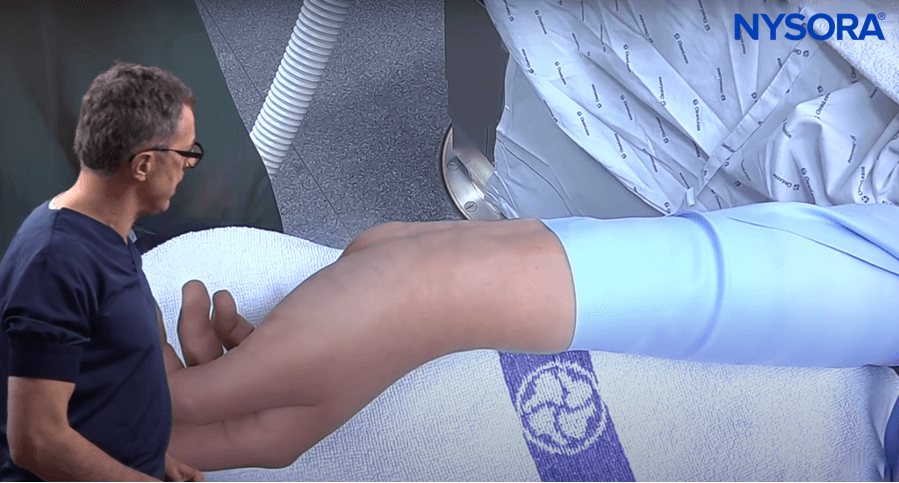
Some peripheral veins at the dorsum of the wrist and hand are becoming visible. Typically, the best veins that you get with this technique are either on the dorsal or volar side of the extremity.

Veins are becoming visible at the dorsum of the wrist and hand.
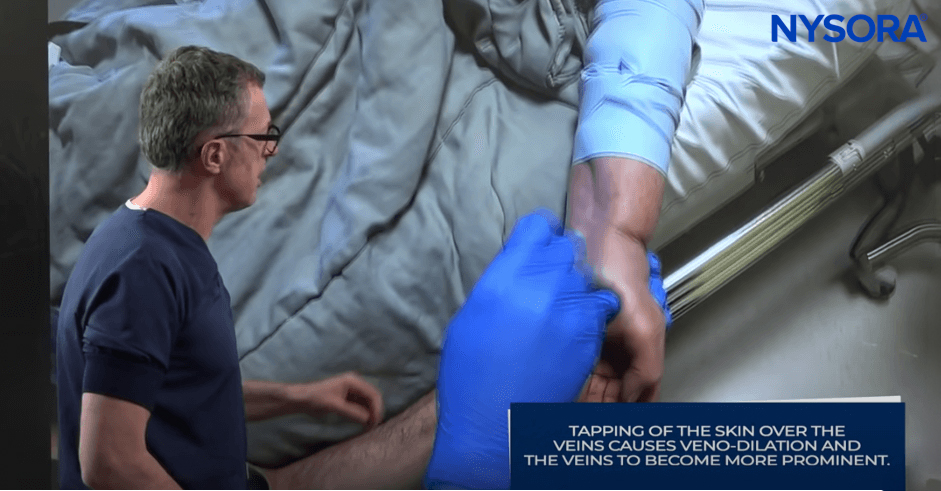
We will tap the skin several times since the tapping releases inflammatory mediators.
We stabilize the skin, stretch it, and, if possible, pick the vein that has two contributors, as that is where the veins are fixed the best.
Now the catheter enters into the vein, and we have an immediate flashback. And voila – another successful intravenous placement!
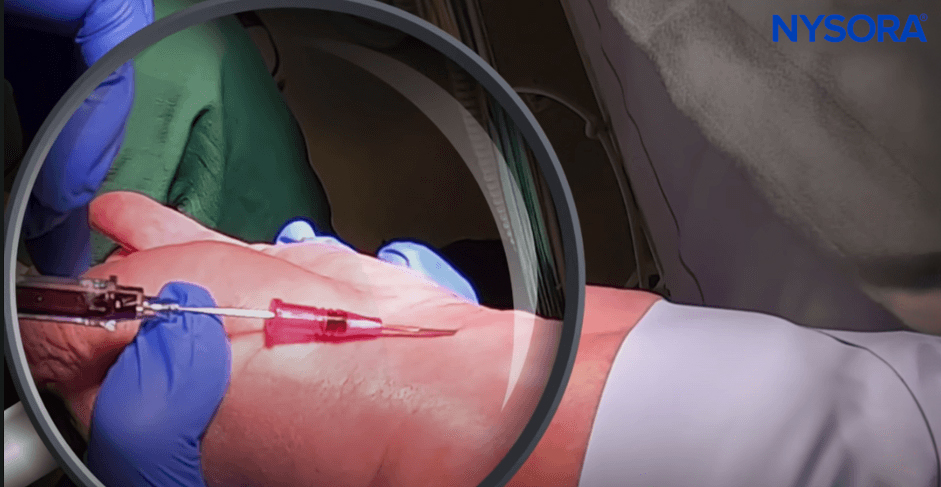
Placed catheter.