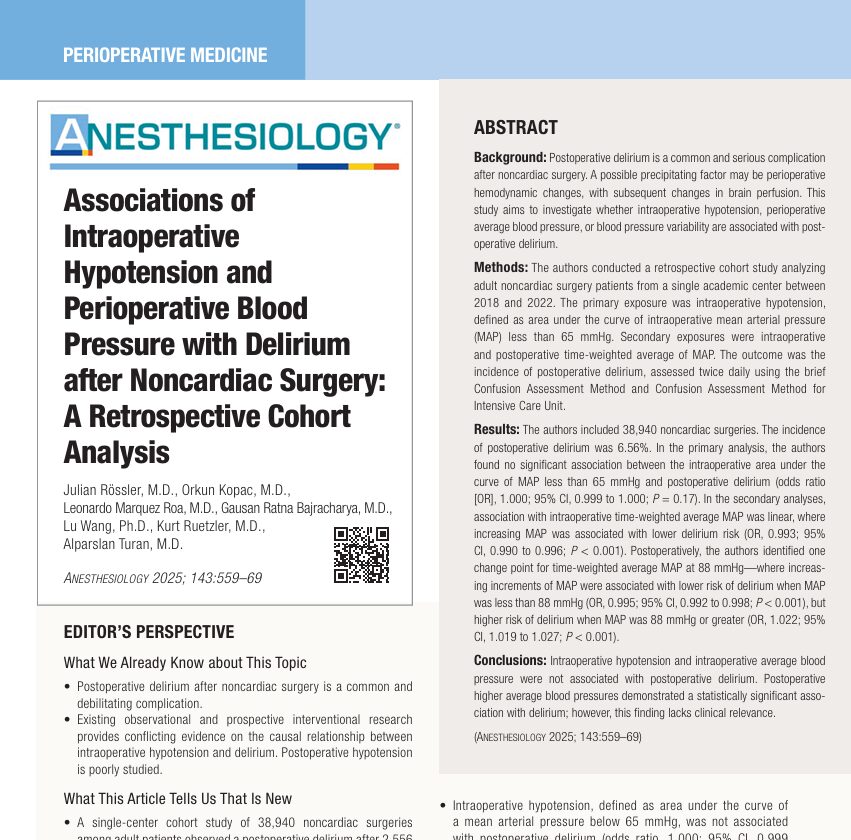




Researchers from the Cleveland Clinic and international collaborators in anesthesiology have released pivotal findings in the September 2025 issue of Anesthesiology that challenge longstanding assumptions about the relationship between blood pressure and postoperative delirium in non-cardiac surgery patients.
Background: What is postoperative delirium?
Postoperative delirium (POD) is an acute and fluctuating disturbance in cognition, consciousness, and attention. It often affects older adults following surgery and is associated with:
- Longer hospital stays
- Increased morbidity and mortality
- Higher healthcare costs
Understanding modifiable risk factors for POD is key to prevention, as effective treatment remains limited.
Study objectives and methodology
What was studied?
- A retrospective cohort study involving 38,940 noncardiac surgeries performed between 2018 and 2022.
- Researchers aimed to determine if intraoperative hypotension or other blood pressure (BP) metrics were linked to POD.
Key metrics:
- Intraoperative hypotension: Defined as the area under the curve (AUC) for mean arterial pressure (MAP) < 65 mmHg.
- Secondary metrics: Time-weighted average MAP (TWA-MAP) intra- and postoperatively.
- Exploratory metrics: Blood pressure variability, including:
- Average real variability (ARV)
- Variability independent of mean (VIM)
- Average real variability (ARV)
Key findings
1. Intraoperative hypotension is not associated with POD
Despite long-held beliefs, the study found no significant relationship between intraoperative hypotension (using MAP < 65 mmHg) and POD, even in patients aged 65+.
2. Intraoperative average MAP showed a weak protective effect
- Linear relationship observed.
- However, the effect size was small, limiting clinical relevance.
3. Postoperative MAP presented a U-shaped relationship
- Risk of delirium:
- Decreased when MAP increased below 88 mmHg.
- Increased when MAP exceeded 88 mmHg.
- Decreased when MAP increased below 88 mmHg.
- This suggests both hypotension and hypertension postoperatively may be problematic.
4. Blood pressure variability has a complex role
- Postoperative variability (ARV and VIM) had a nonlinear relationship with POD:
- Low variability: associated with reduced risk.
- High variability: associated with increased risk.
- Low variability: associated with reduced risk.
- This aligns with concerns about cerebral autoregulation disruptions.
Clinical implications
What do these results mean for anesthesiologists?
- Intraoperative BP management: Aggressively avoiding hypotension based on the 65 mmHg MAP threshold may not reduce POD risk.
- Postoperative BP trends deserve more attention; both elevated and highly variable BPs may be harmful.
- Blood pressure variability may be a more critical factor than previously recognized.
Conclusion
This large-scale study challenges the assumption that intraoperative hypotension, defined as MAP < 65 mmHg, directly contributes to postoperative delirium. Instead, the focus may need to shift toward postoperative BP trends and variability as more clinically relevant factors.
Reference: Rössler J et al. Associations of Intraoperative Hypotension and Perioperative Blood Pressure with Delirium after Noncardiac Surgery: A Retrospective Cohort Analysis. Anesthesiology. 2025;143:559-569.
Read more about this topic in the Anesthesia Updates section of the Anesthesia Assistant App. Prefer a physical copy? Get the latest literature and guidelines in book format. For an interactive digital experience, check out the Anesthesia Updates Module on NYSORA360!