Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About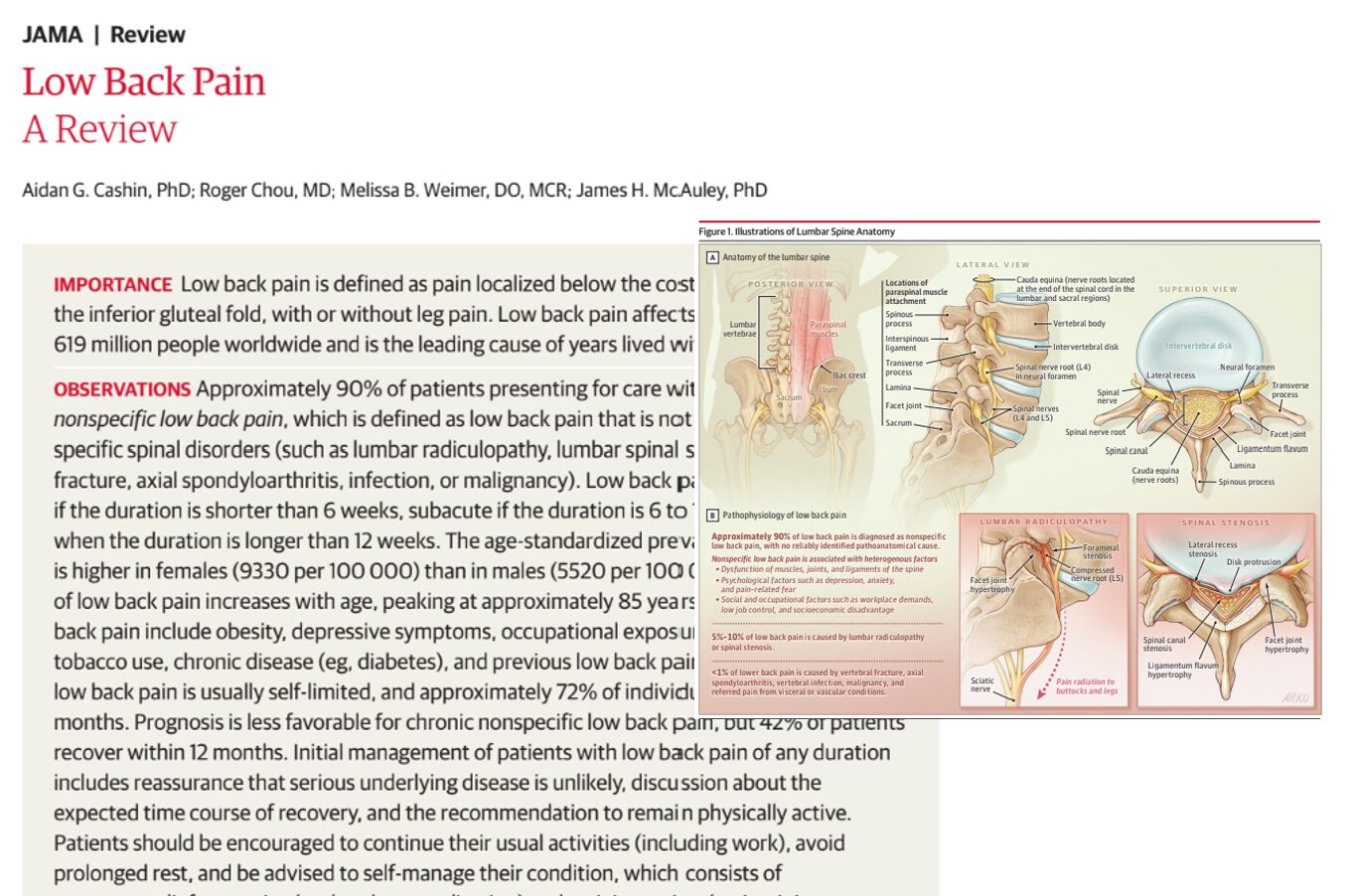





Introduction
Low back pain continues to be one of the most common health conditions worldwide and remains the leading cause of years lived with disability. A major new review published in JAMA provides an updated overview of the epidemiology, diagnosis, prognosis, and treatment of low back pain, offering important insights for clinicians and patients alike.
According to the review, approximately 619 million people worldwide were living with low back pain in 2020. The condition affects people of all ages, becomes more common with advancing age, and is more prevalent among women than men.
The review emphasizes that while low back pain is extremely common, most cases are not caused by serious disease. Instead, about 90% of patients have nonspecific low back pain, meaning no single anatomical structure can be reliably identified as the source of symptoms.
What is low back pain?
Low back pain is defined as pain located below the rib cage (costal margin) and above the gluteal folds, with or without associated leg pain.
The condition is typically classified according to symptom duration:
- Acute low back pain: less than 6 weeks
- Subacute low back pain: 6 to 12 weeks
- Chronic low back pain: longer than 12 weeks
Most patients seen in primary care do not have a serious underlying spinal disorder. Specific causes such as vertebral fracture, spinal infection, malignancy, inflammatory disease, or cauda equina syndrome are relatively uncommon.
Why is low back pain so common?
Researchers note that low back pain is a complex biopsychosocial condition.
Rather than being caused by a single damaged structure, symptoms often arise from an interaction between:
- Biological factors
- Psychological factors
- Social influences
- Occupational demands
- Lifestyle factors
Major risk factors identified
Several factors increase the likelihood of developing low back pain.
Lifestyle and health factors
Occupational factors
- Heavy lifting
- Repetitive physical work
- High workplace demands
- Low job control
Demographic factors
- Increasing age
- Female sex
The prevalence rises steadily with age and peaks around 85 years.
Symptoms patients commonly experience
Patients typically report:
- Pain in the lower back
- Difficulty bending
- Difficulty lifting objects
- Problems walking
- Reduced tolerance for sitting
- Reduced tolerance for standing
- Functional limitations at home and work
Pain may radiate into the buttock or thigh but often does not follow a specific nerve-root distribution.
Many patients experience symptom fluctuations, with pain worsening during certain activities and improving after movement modification or rest.
When should clinicians be concerned?
Red flags for serious spinal disease
- History of cancer
- Fever
- Recent spinal infection
- Intravenous drug use
- Significant trauma
- Osteoporosis
- Long-term corticosteroid use
- Progressive neurological deficits
- New bowel dysfunction
- New bladder dysfunction
- Saddle anesthesia
Imaging is often unnecessary
One of the strongest messages from the review is that routine imaging should not be performed for most patients with nonspecific low back pain.
Researchers note that MRI and X-ray findings frequently reveal age-related degenerative changes even in people without symptoms.
Common findings include:
- Disc degeneration
- Disc bulges
- Facet arthropathy
- Endplate changes
These findings can lead to:
- Increased anxiety
- Unnecessary testing
- Inappropriate treatments
- Misattribution of symptoms
The review therefore recommends reserving imaging for patients with red-flag symptoms or specific clinical indications.
Prognosis: what happens over time?
Acute low back pain
The outlook is generally favorable.
Approximately:
- 72% of patients recover within 12 months
- Most improvement occurs within the first 6 weeks
Chronic low back pain
The prognosis is less optimistic.
Researchers found that:
- Only 42% recover within 12 months
- Many continue to experience persistent symptoms beyond one year
However, meaningful improvements in function and quality of life remain achievable even when pain persists.
First-line treatment for acute low back pain
The review highlights several evidence-based treatments for acute nonspecific low back pain.
Step 1: reassure the patient
Patients should be informed that:
- Serious disease is unlikely.
- Recovery is usually favorable.
- Remaining active is important.
- Bed rest should be avoided.
Step 2: encourage self-management
Self-management strategies include:
- Heat application
- Activity pacing
- Continuing daily activities
- Maintaining work participation when possible
Step 3: consider nonpharmacological therapies
Recommended options include:
- Superficial heat
- Spinal manipulation
- Massage
- Acupuncture
Step 4: medications when needed
Recommended medications include:
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Skeletal muscle relaxants
Examples cited in the review include ibuprofen, naproxen, celecoxib, cyclobenzaprine, and tizanidine.
What treatments are not recommended?
Several commonly used treatments showed limited benefit.
Acute pain
Not routinely recommended:
- Acetaminophen (paracetamol) alone
- Benzodiazepines
- Systemic corticosteroids
Chronic pain
Not recommended because of limited efficacy or increased risks:
- Long-term opioids
- Antiepileptic medications
- Routine corticosteroids
- Routine skeletal muscle relaxants
- Transcutaneous electrical nerve stimulation (TENS)
- Lumbar supports
- Therapeutic ultrasound
Best treatments for chronic low back pain
For chronic low back pain, the emphasis shifts away from medication and toward active rehabilitation.
Exercise remains the cornerstone
Researchers found benefits from:
- Strength training
- Aerobic exercise
- Pilates
- Flexibility programs
- Combined exercise approaches
Importantly, no single exercise type appears superior.
The best program is often the one patients enjoy and can consistently perform.
Psychological therapies matter
Evidence supports:
- Cognitive behavioral therapy (CBT)
- Pain education
- Mindfulness-based approaches
- Cognitive functional therapy
These therapies help patients address fear of movement, maladaptive beliefs, and behavioral patterns that contribute to persistent disability.
Multidisciplinary care
Integrated programs combining:
- Exercise
- Psychological treatment
- Vocational support
- Medical management
appear to provide the greatest overall benefit for many patients with chronic symptoms.
Surgery and invasive procedures: limited role
The review found little evidence supporting invasive procedures for nonspecific chronic low back pain.
Procedures generally not recommended
- Epidural steroid injections
- Facet joint injections
- Routine spinal cord stimulation
- Routine spinal fusion surgery
- Disc replacement surgery
These interventions should only be considered in carefully selected patients after extensive conservative treatment has failed.
Key takeaways
- Low back pain affects approximately 619 million people globally.
- About 90% of cases are nonspecific low back pain.
- Routine imaging is usually unnecessary.
- Staying active is a cornerstone of treatment.
- Heat, massage, spinal manipulation, acupuncture, NSAIDs, and muscle relaxants can help acute pain.
- Exercise and psychological therapies are first-line treatments for chronic pain.
- Multidisciplinary care offers additional benefits.
- Most invasive procedures provide limited value for nonspecific low back pain.
- Long-term opioid therapy should generally be avoided.
Conclusion
The 2026 JAMA review reinforces a growing consensus in musculoskeletal medicine: most low back pain is not a structural problem requiring scans, injections, or surgery. Instead, successful management focuses on education, self-management, physical activity, exercise, and addressing psychological and social contributors to pain.
Reference: Cashin AG et al. Low Back Pain: A Review. JAMA. Published online June 15, 2026.
Read more about recent evidence like this in NYSORA’s Anesthesia Assistant app. Simulate case, check dosages and search through NYSORA knowledge database!