Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Define and describe autonomic dysreflexia
- Recognize signs and symptoms of autonomic dysreflexia
- Manage patients with autonomic dysreflexia
Definition & mechanisms
- Autonomic dysreflexia is a condition that emerges after a spinal cord injury, usually when the damage has occurred above the T6 level
- Dysregulation of the autonomic nervous system leads to an uncoordinated sympathetic response that may result in a potentially life-threatening hypertensive episode when there is a noxious stimulus below the level of the spinal cord injury
- Noxious stimuli consist usually of bladder or bowel distension
- The higher the injury, the greater the severity of the cardiovascular dysfunction
- Significantly increased risk of stroke by 300% to 400%
Signs & symptoms
- Severe headache
- Hypertension
- Piloerection above the level of injury
- Bradycardia
- Facial flushing
- Pallor
- Cold skin
- Sweating in the lower part of the body
- Visual disturbances
- Constricted pupils
- Nasal stuffiness
- Anxiety or feelings of doom
- Nausea and vomiting
- Dizziness
Evaluation
- Identify patients at risk (injury above T6)
- Document baseline blood pressure
- When severe headache occurs, measure blood pressure
- A systolic blood pressure >150 mmHg or >40 mmHg above baseline is indicative of autonomic dysreflexia
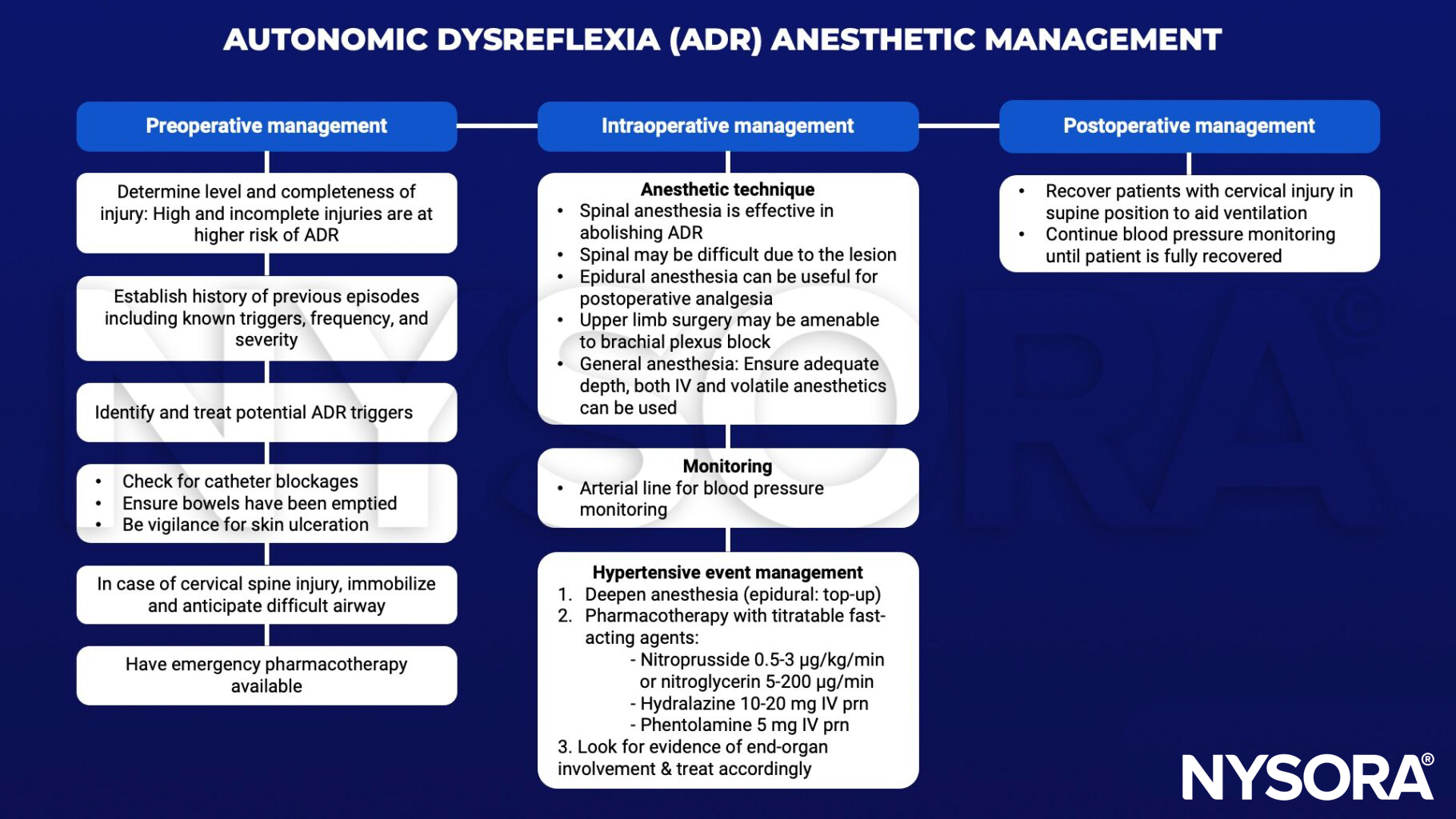
Anesthetic management
Suggested reading
- Allen KJ, Leslie SW. Autonomic Dysreflexia. [Updated 2022 Nov 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482434/
- Petsas A, Drake J. Perioperative management for patients with a chronic spinal cord injury. BJA Education. 2015;15(3):123-30.