Indications
Puncture of free intraperitoneal fluid or ascites can be indicated for diagnostic or therapeutic purposes. Ascites can be caused by:
- Liver disease
- Heart disease
- Malignancy
- Kidney disease
- Chronic inflammation (e.g., pancreatitis)
- Hypoalbuminemia
Note
Understanding free intraperitoneal fluid scanning is essential to perform safe paracentesis.
Procedure
Ultrasound can be used to determine the site of puncture and guide the needle to decrease the risk of vessel or bowel injury. A curvilinear transducer is typically used to assess the presence of free fluid. A linear transducer is used for ultrasound-guided puncture of the free fluid.
- Position the patient supine with the head 30 degrees elevated (this will allow the fluid to collect in the lower quadrants).
- Scan with a curvilinear transducer the LUQ, RUQ, and pelvic areas, to assess the presence and the amount of free fluid. Then scan both lateral lower quadrants and identify an ‘ideal’ insertion area. The space where there is enough free fluid between the abdominal wall and the viscera is called ‘a pocket’.
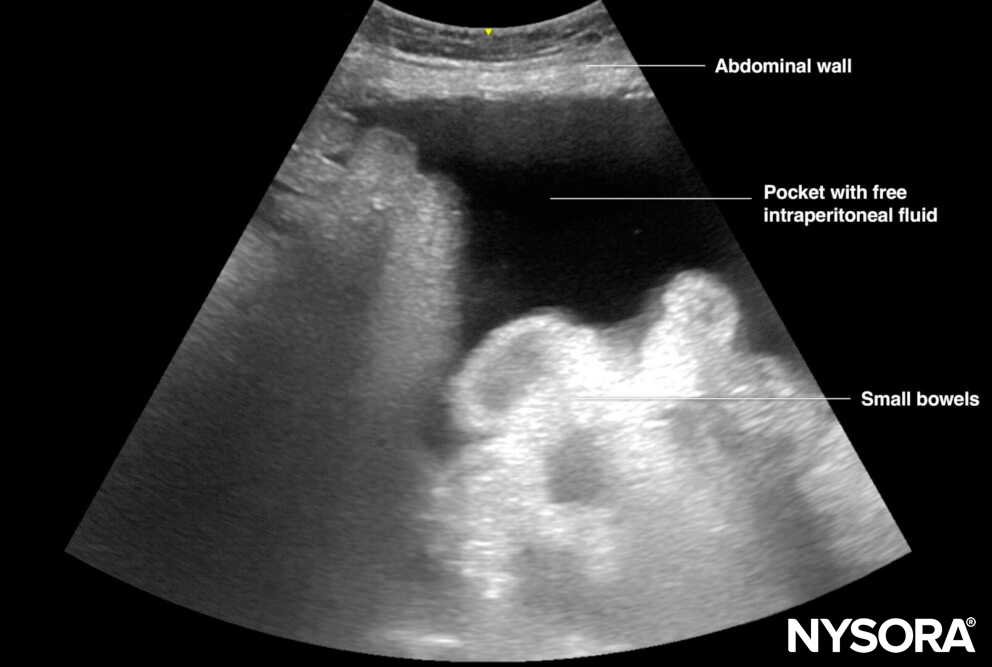
Illustration of a pocket with free intraperitoneal fluid.
- After identification of a pocket, switch to a linear transducer and scan the area of interest. Adjust the depth setting and focus, where available, to visualize underlying visceral structures at all times.
Tip
Use color Doppler to identify the blood vessels of the abdominal wall and decrease the risk of vascular puncture. The optimal needle insertion site provides adequate space between the abdominal wall and the viscera, with no major blood vessels in the needle’s path.
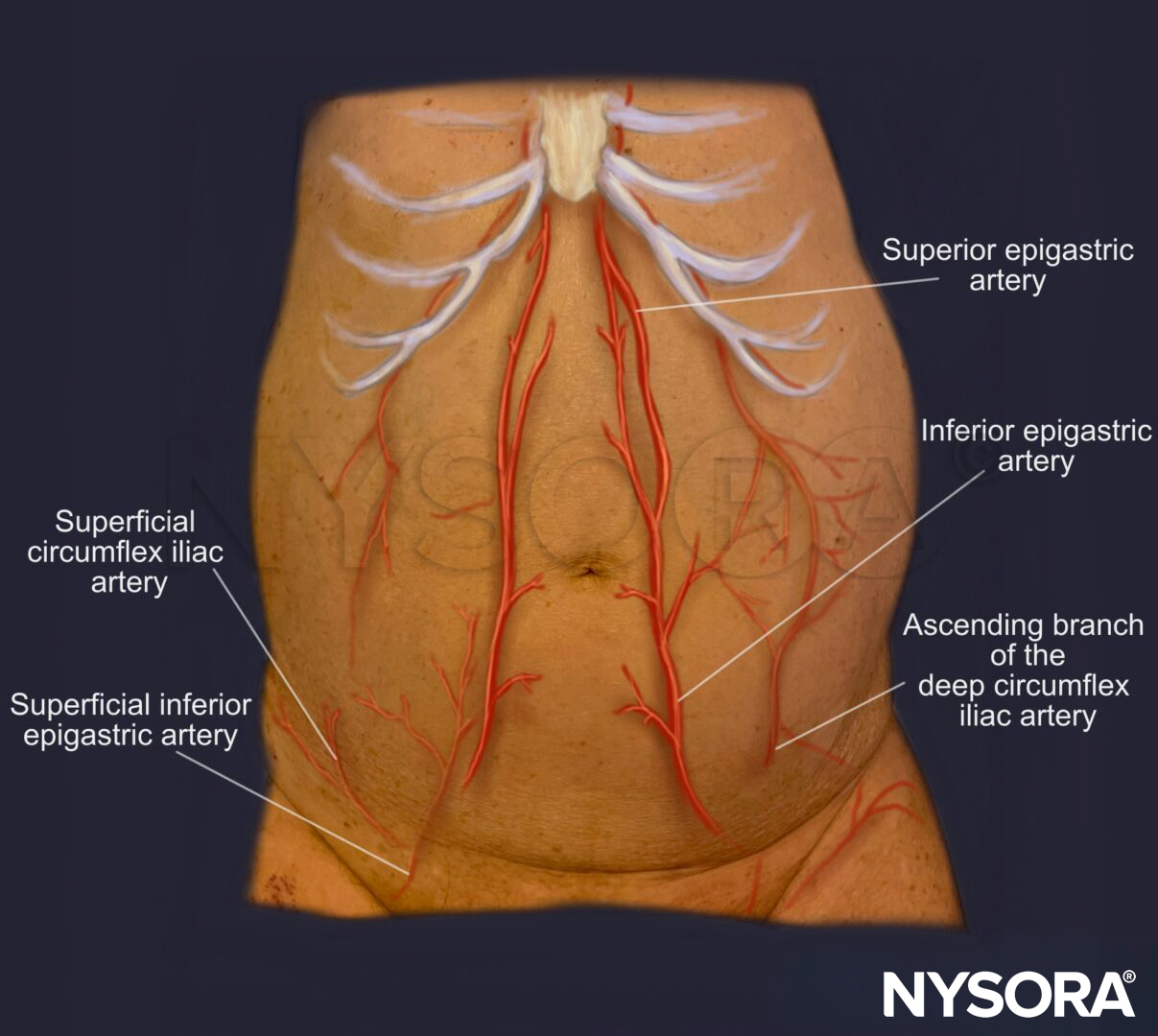
Arterial blood supply of the abdominal wall.
- Insert the needle in-plane from a lateral to medial direction.

In-plane insertion of a needle during paracentesis in the LLQ.
Tips
- Ultrasound-guided paracentesis reduces the risk of bleeding at the insertion site, puncture site infection, and abdominal wall hematoma.
- Ultrasound helps identify and avoid puncturing the dilated veins (caput Medusa) in patients with ascites.
- Look for and avoid the inferior epigastric artery, which is usually located 5-6 cm lateral to the midline by using color Doppler.
- Avoid needle insertion through the suprapubic area due to the vicinity of the urinary bladder.
- Keep in mind that the visceral structures (bowels) move autonomously, contain air, and therefore tend to float up. Therefore, during needle insertion, monitor floating structures to reduce the risk of bowel puncture and needle contamination.
Clinical updates
Wubben et al. (POCUS Journal, 2024) retrospectively analyzed 131 ED paracenteses and found that emergency physicians achieved similar success with ultrasound-guided (real-time) versus ultrasound-assisted techniques (97.7% vs 95.6%, p=0.503), with no fatal complications. Good in-plane needle visualization was documented in 58% of real-time cases, and all four procedural failures occurred with curvilinear probes, whereas none occurred with a linear transducer. Complication rates were low (10.5% guided vs 4.4% assisted, p=0.238), with ascites leak most common, supporting real-time guidance as feasible and recommending linear probe use with vessel identification to optimize safety.
- Wubben BM, Dandashi J, Rizvi O, Adhikari S. Emergency Physician Performed Ultrasound-Guided Abdominal Paracentesis: A Retrospective Analysis. POCUS J. 2024;9(1):75-79. Published 2024 Apr 22.