
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the fluid compartments and the distribution of fluid and electrolytes
- Manage the fluid and electrolyte balance in surgical patients
Background
- Body water content varies with age and gender:
TBW (% body weight) ICF (% body weight) ECF (% body weight)
Neonate 75 40 35
Infant 70 40 30
Adult male 60 40 20
Adult female 55 35 20
Elderly female 45 30 15
- Approximately two-thirds of total body water (TBW) is intracellular fluid (ICF) and one-third is extracellular fluid (ECF)
- ECF is further divided into interstitial fluid (ISF) and plasma
TBW and electrolyte distribution
- Example of TBW and electrolyte distribution in a healthy 70-kg man:
ICF Interstitial fluid Plasma
Water (L) 28 11 3
Na+ (mmol/L) 10 140 140
K+ (mmol/L) 150 4 4
Ca2+ (mmol/L) / 2.5 2.5
Mg2+ (mmol/L) 26 1.5 1.5
Cl- / 114 114
HCO3- 10 25 25
HPO4(2-) 38 1 1
So4(2-) / 0.5 0.5
Prot- 74 2 16
Redistribution of infused fluids
- The redistribution of infused fluids depends on their composition relative to that of each compartment:
ICF(%) Interstitial fluid (%) Plasma (%)
Saline (0.9% 0 79 21
Dextrose (5%) 67 26 7
Homeostasis maintenance
- Homeostasis maintenance requirements for surgical patients:
- Water: 25-30 mL/kg/day for adults (use ideal body weight for obese patients)
- Sodium: 1 mmol/kg/day, can be administered by:
- 2500 mL of 4% dextrose/0.18% saline over 24 hours
- 2000 mL of 5% dextrose and 500 ml of 0.9% saline over 24 hours
- Potassium: 1 mmol/kg/day
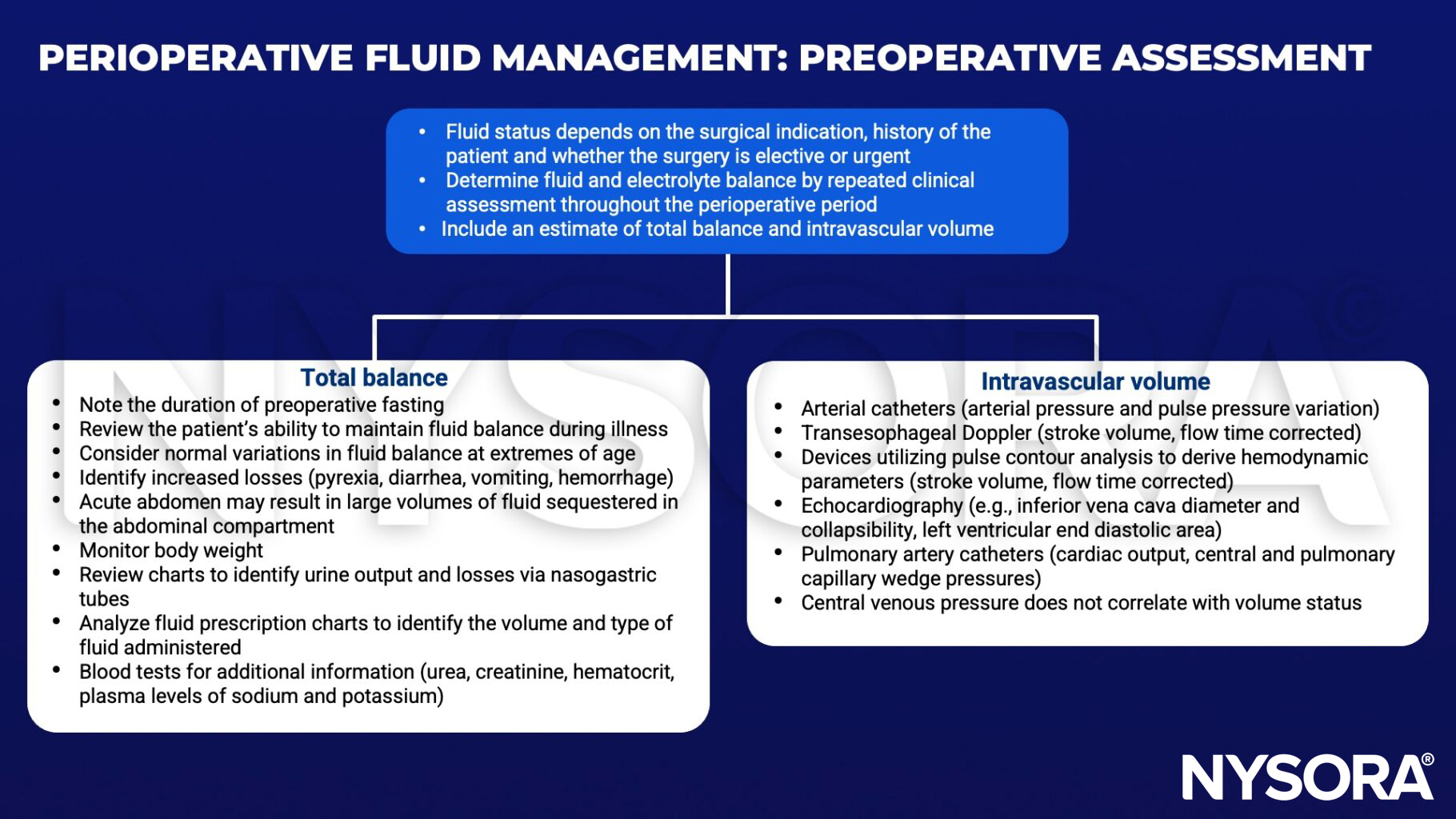
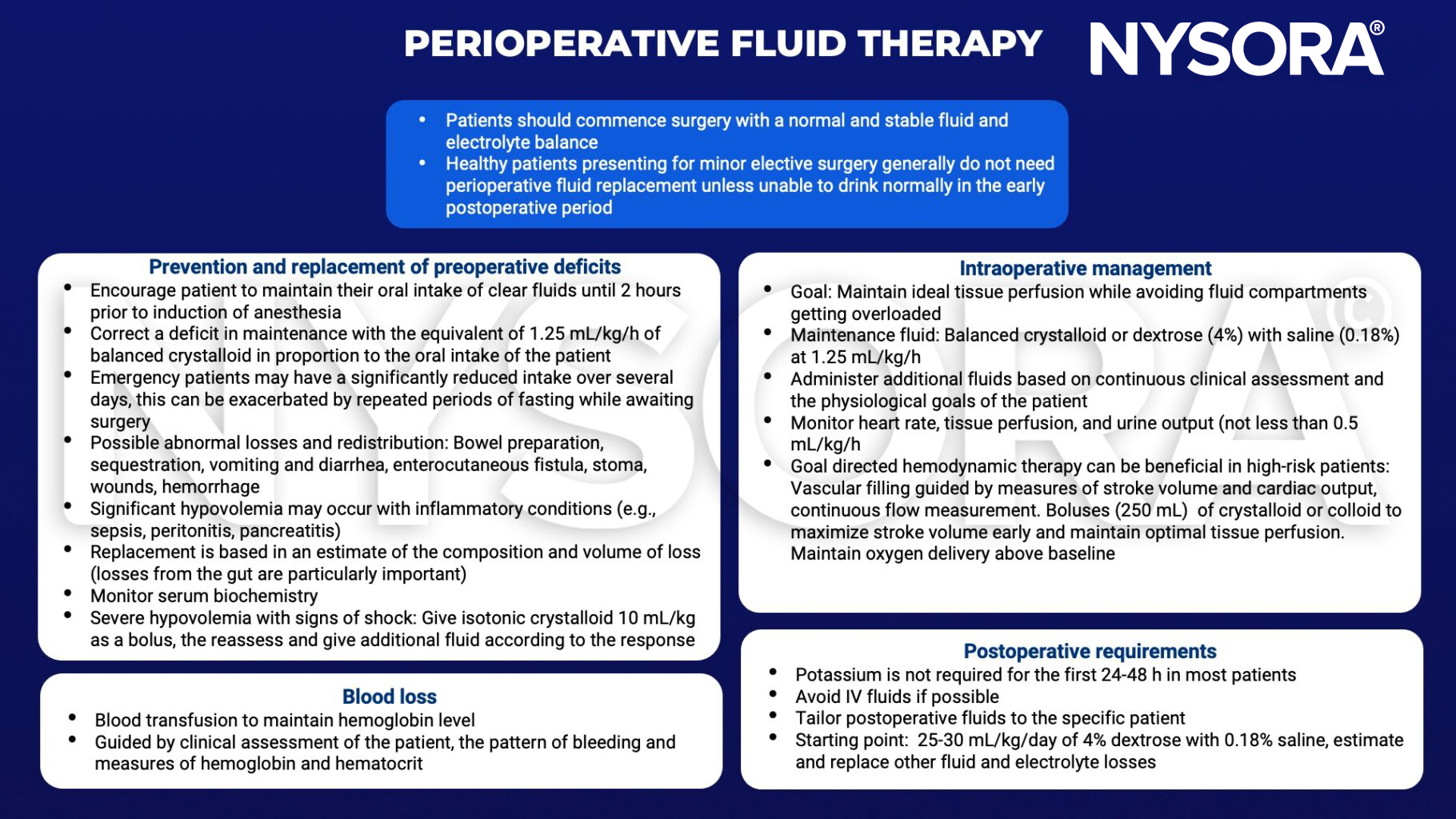
Perioperative fluid management
Suggested reading
- Pollard BJ, Kitchen, G. Handbook of Clinical Anaesthesia. Fourth Edition. CRC Press. 2018. 978-1-4987-6289-2.
- Rassam SS, Counsell DJ. Perioperative electrolyte and fluid balance. Continuing Education in Anaesthesia Critical Care & Pain. 2005;5(5):157-60.
Clinical updates
Markl-Le Levé et al. (Current Opinion in Anaesthesiology, 2025) describe a paradigm shift in hemorrhagic shock resuscitation away from liberal crystalloid and colloid administration toward restrictive, physiology-guided strategies that prioritize preservation of coagulation, endothelial integrity, and microcirculatory flow. The review highlights that balanced crystalloids are preferred over saline for initial resuscitation, while hydroxyethyl starch and albumin are no longer recommended due to renal, coagulation, and mortality concerns, and plasma should not be used solely for volume replacement.
- Read more about this study HERE.
Diz et al. (A&A, 2025) report, in a meta-analysis of 15 randomized trials including over 35,000 critically ill adults, that balanced crystalloids are associated with lower 90-day mortality than normal saline in non–traumatic brain injury (TBI) patients but with higher mortality in patients with TBI. Renal outcomes, length of stay, and need for organ support were similar between fluids, highlighting that electrolyte composition and buffering matter most in specific physiological contexts rather than universally.
- Read more about this study HERE.
Coppola et al. (BJA, 2025) review the physiological basis and clinical application of diuretics in critically ill patients, emphasizing that loop diuretics reliably increase urine output but do not improve mortality or renal replacement therapy requirements and frequently cause electrolyte and acid–base disturbances. The review highlights that diuretic resistance is common and can be mitigated with continuous infusions or combination therapy (thiazides or acetazolamide), while routine albumin co-administration is not supported by evidence.
- Read more about this study HERE.
A large prospective study by Andersson et al. (BJA, 2025) demonstrates that a balanced isotonic electrolyte solution containing 1% glucose safely maintains intraoperative glucose and electrolyte homeostasis in infants aged 1–12 months, with no episodes of hypoglycemia and only rare, mild hyperglycemia or hyponatremia. Across 365 infants, plasma glucose remained stable or increased modestly, sodium and acid–base changes were clinically insignificant, and ketosis remained mild even with prolonged fasting.
- Read more about this study HERE.









