Indications
- Delivery of specific drugs, drug infusions, or long-term therapy
- Fluid resuscitation
- Hemodialysis
- Monitoring of central venous pressure
Considerations
- Coagulopathy
- Infection at the insertion site
- Underlying thrombosis
Tip
Check the patient’s chart with special attention to the laboratory results for coagulation disorders and the chest X-ray for possible previously inserted materials before the start of the procedure (if available)
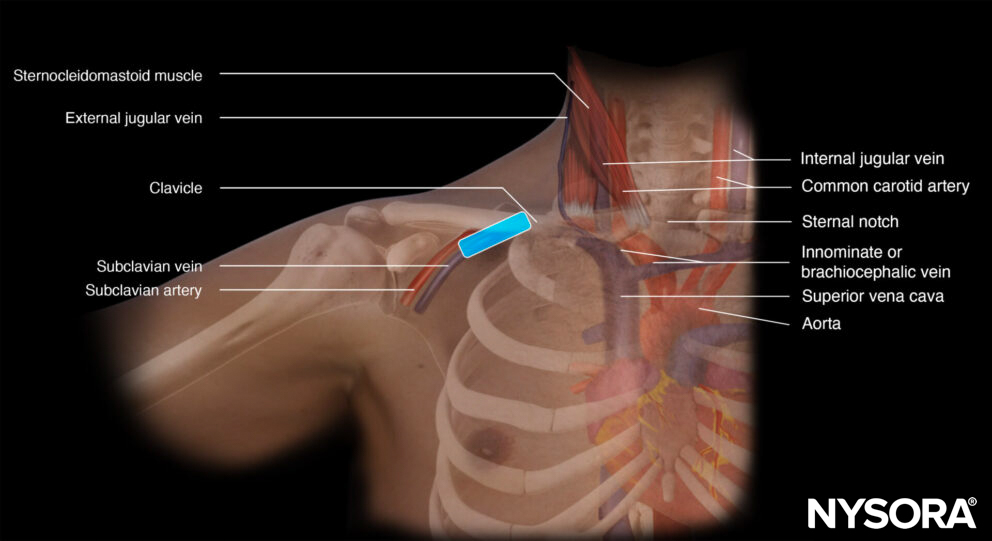
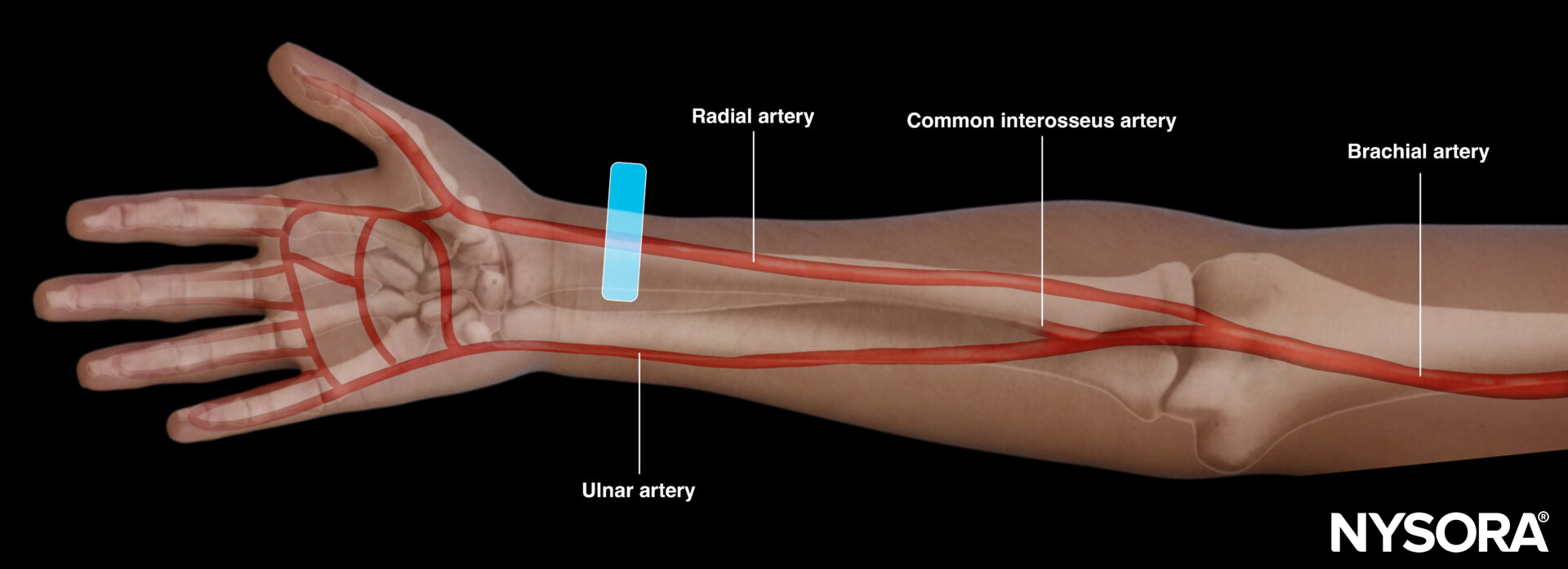
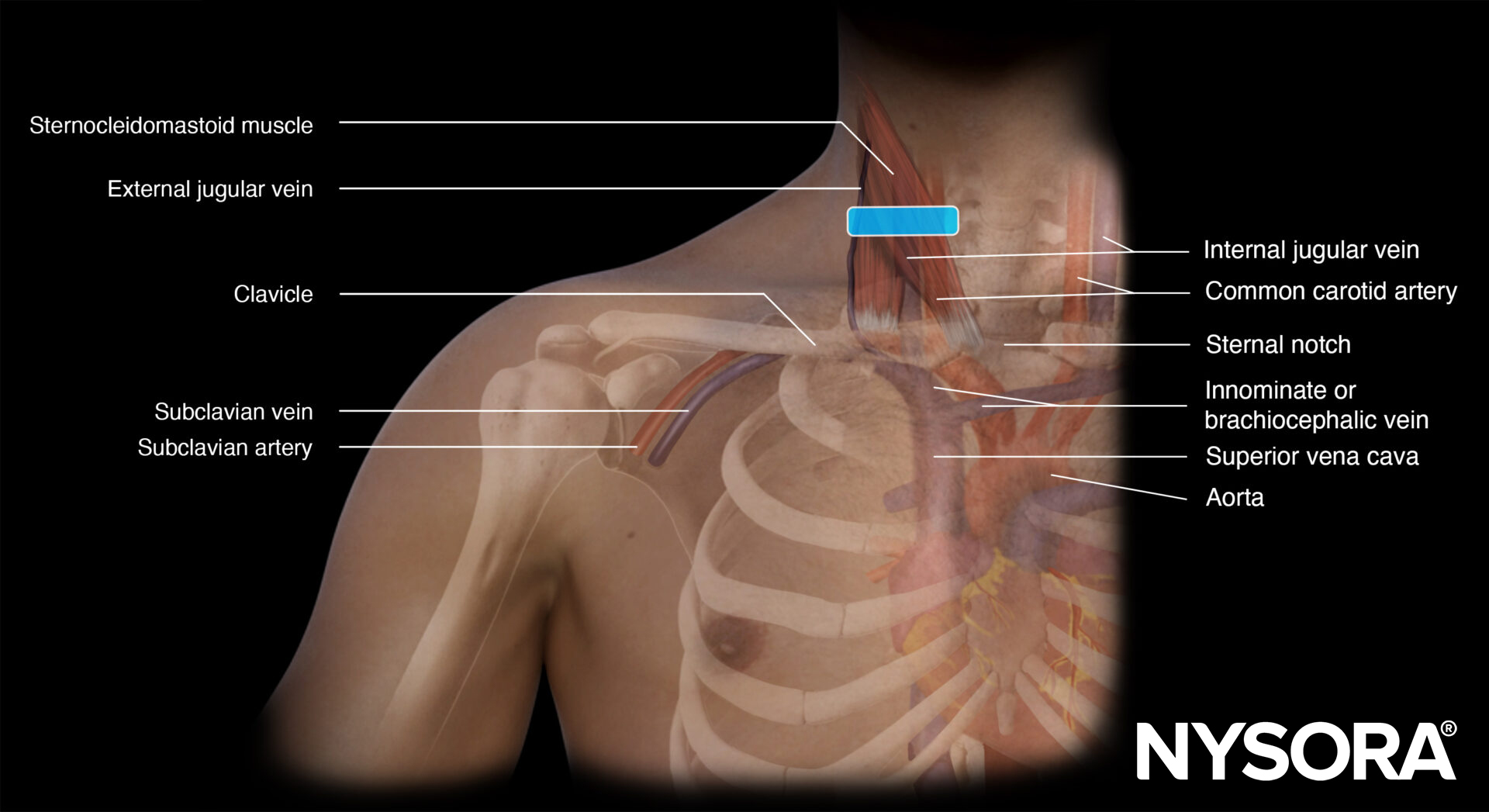
Functional anatomy
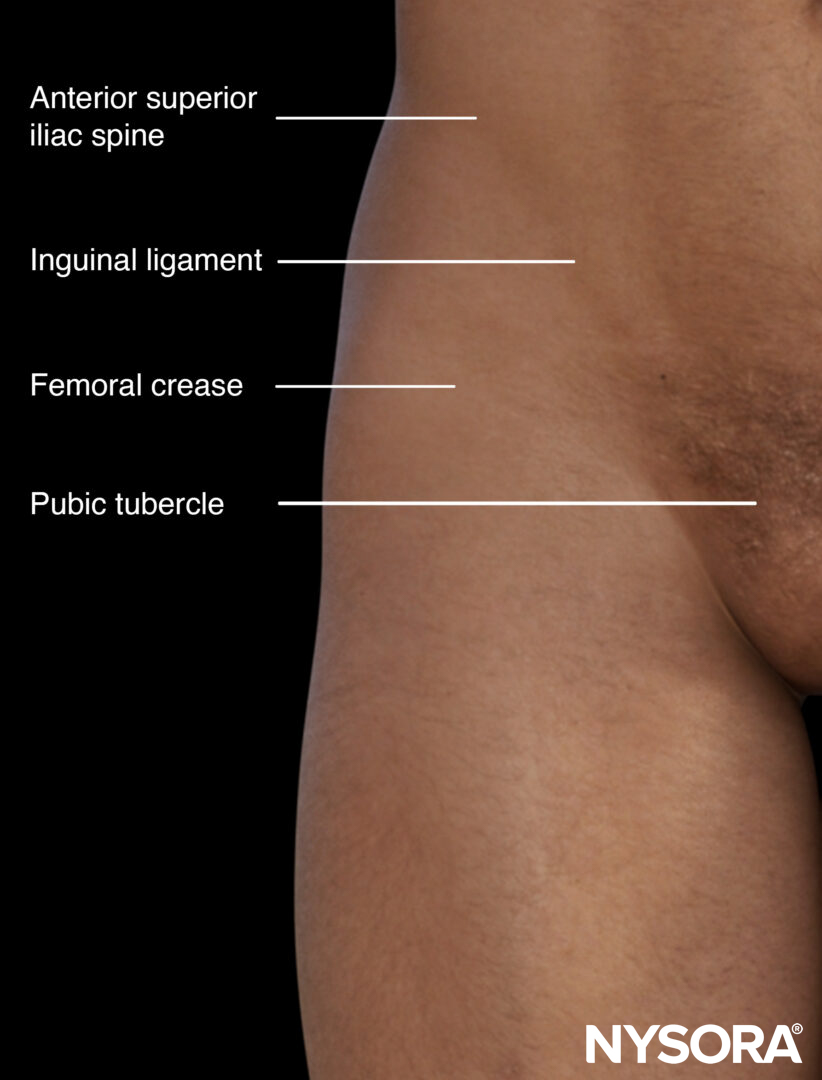
External anatomy relevant to the puncture of the femoral vein.
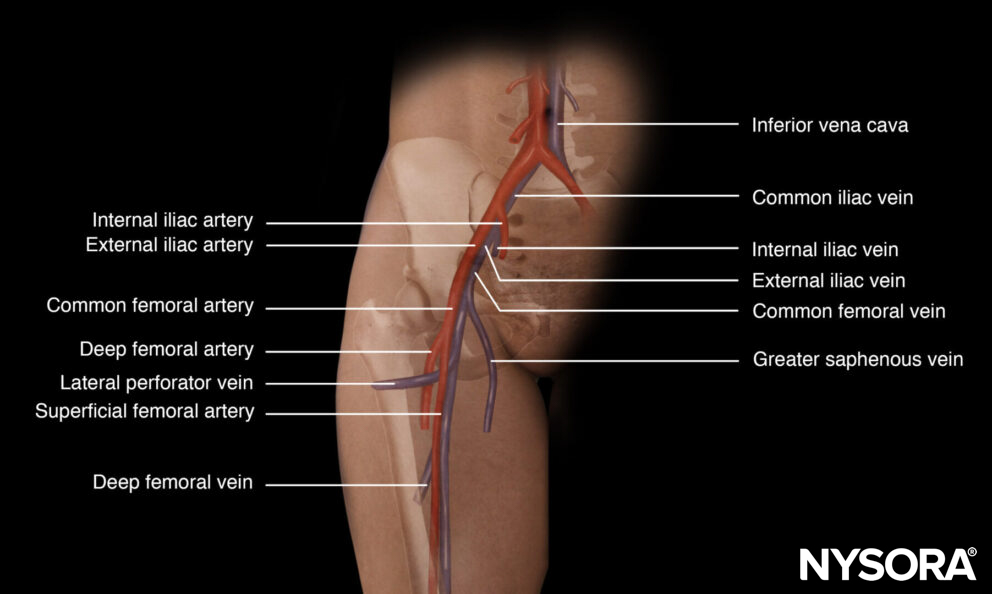
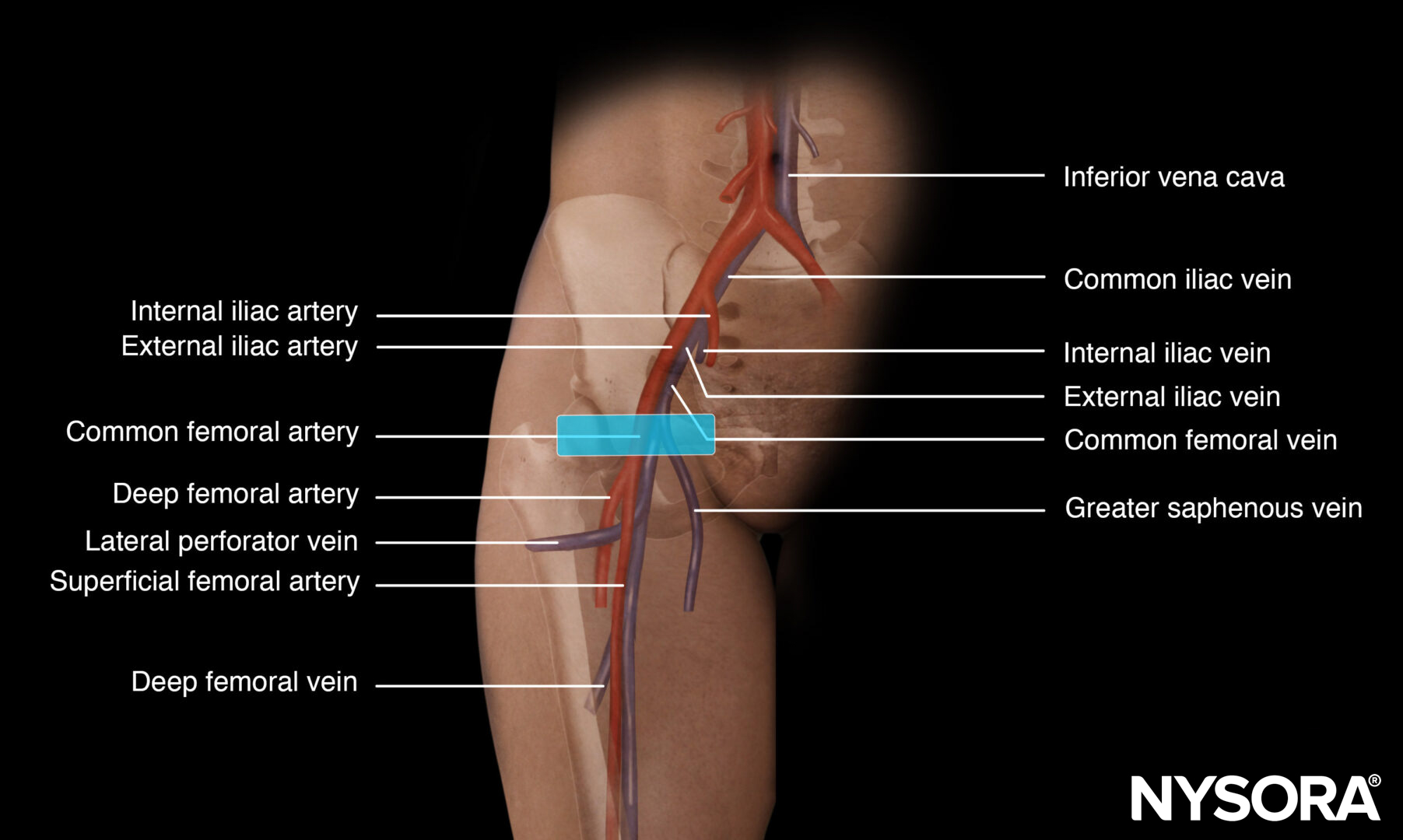
Anatomy of the femoral vein.
Preparation
- Make sure that there is a nurse or physician to assist you with the procedure.
- It is advisable to use a box or a set containing all the necessary materials for central line insertion.
- A central line insertion is a complex procedure that requires a stepwise and systematic approach. This will be described in the ‘Technique’ section.
- Full ASA monitoring should be applied, as clinical information is important and relevant (e.g., desaturation, pulsatile red blood, right ventricular stimulation).
Patient position
Supine position with the ipsilateral leg in slight abduction and external rotation.

Patient position for a femoral vein cannulation.
Note
Reverse Trendelenburg can also be considered for femoral vein distention.
Technique
General steps for central line placement
- Wear a mask and a surgical hat before starting the procedure
- Scrub
- Wear a sterile gown and sterile gloves
- Disinfect the area of interest (2% chlorhexidine in 70% isopropyl alcohol)
- Use sterile drapes to cover non-sterile areas
- Prepare the central line set (flush all lumens with saline and close all lumens except for the one that threads the guidewire)
- Use a sleeve to cover the ultrasound transducer
- Apply sterile gel to the patient’s skin
- Identify the vein of interest
- Freeze the skin under ultrasound guidance with 5 mL of lidocaine 2% if the patient is awake
- Introduce the needle with ultrasound guidance into the lumen of the internal jugular, femoral, or subclavian vein by using the creep technique
- Thread the guidewire when the needle tip is in the middle of the lumen of the vein
- Hold the guidewire at all times and slide the needle backward over the guidewire
- Confirm the position of the guidewire with ultrasound
- Make a small slip into the skin next to the guidewire with a surgical knife
- Dilate the skin while holding the guidewire
- Thread the catheter over the guidewire and hold the guidewire at all times
- When the catheter is in the right position, pull out the guidewire and check all lumens for positive blood aspiration
- Flush all lumens with saline
- Suture the catheter to the skin
- Apply a sterile dressing
Femoral vein cannulation
For femoral vein cannulation, a similar position of the transducer is obtained as for femoral artery cannulation. Place the transducer on the medial third of the line that connects the pubic tubercle with the anterior superior iliac spine or the inguinal ligament. Then scan 1-2 cm distal for the actual puncture.
Transducer position for femoral vein cannulation.
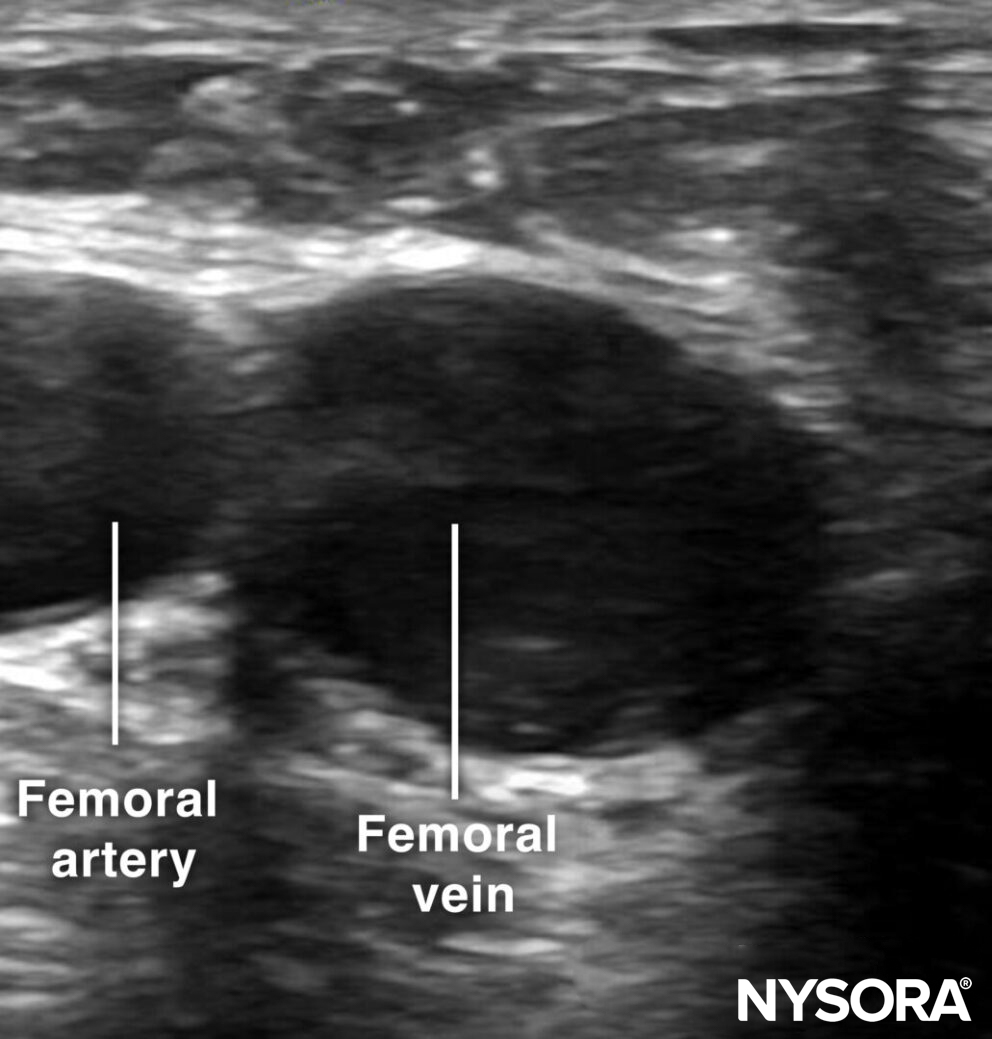
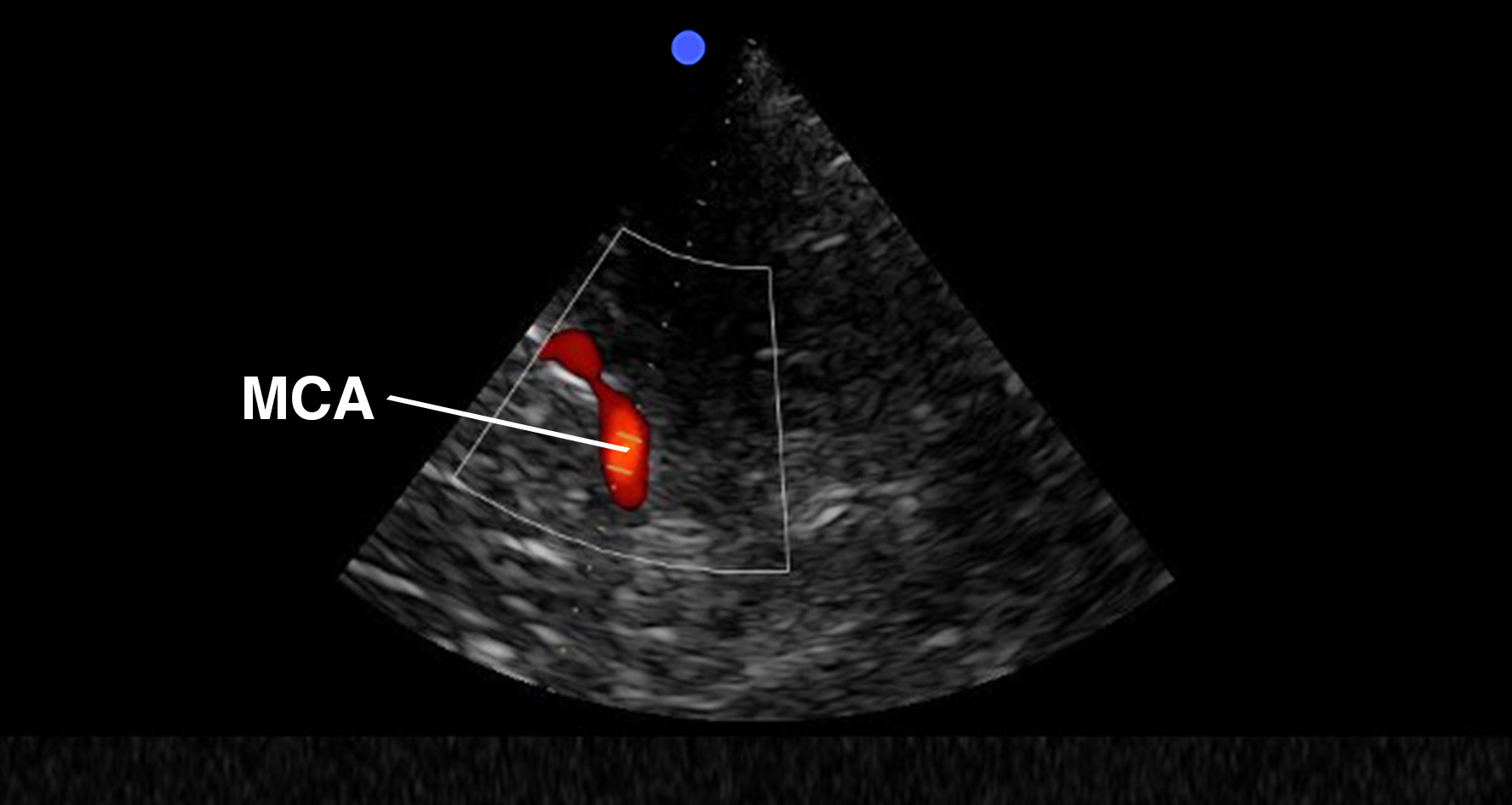
Sonoanatomy for femoral vein cannulation.
The femoral vein is approached just distal to the inguinal ligament by an out-of-plane technique. Use the creep technique to follow the needle tip at all times.
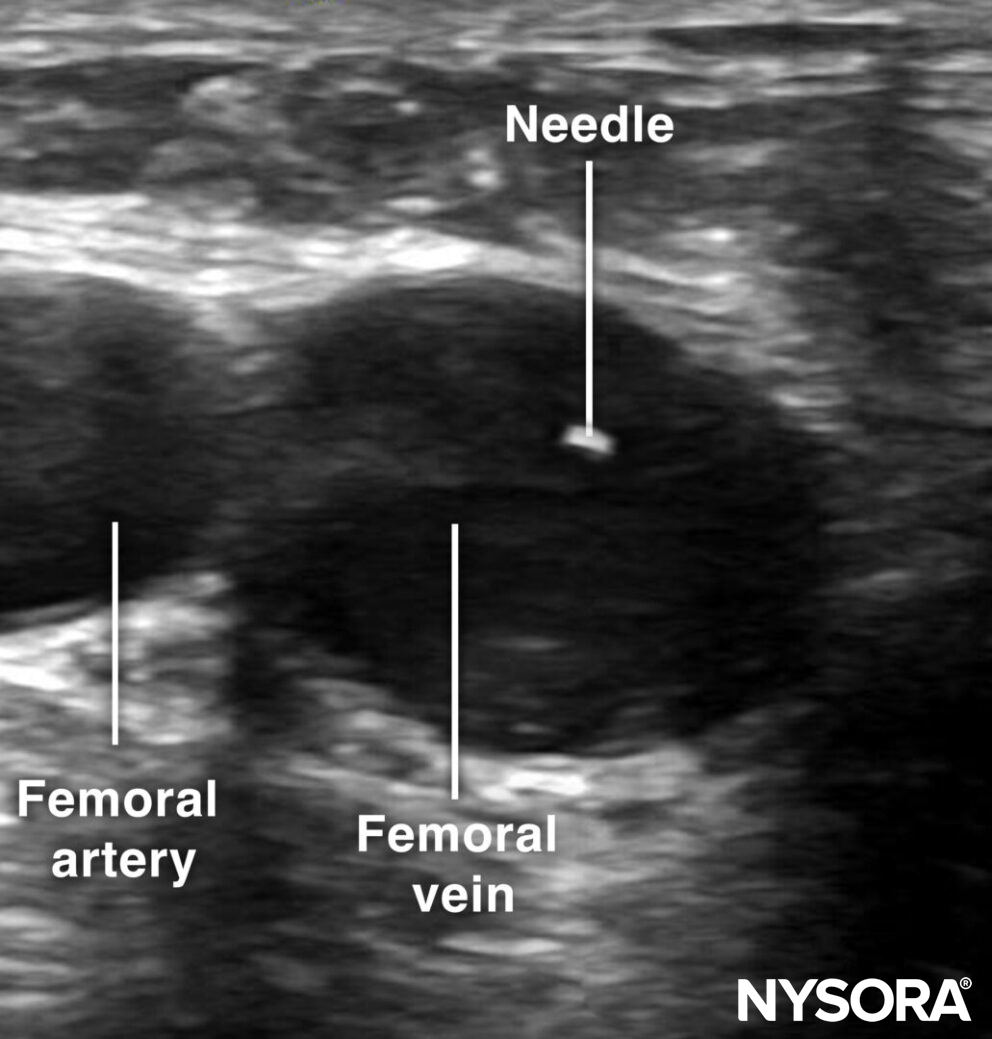
Out-of-plane cannulation of the femoral vein.
Tips
- Ultrasound-guided central venous access reduces complication rates compared to a blind technique.
- Femoral vein cannulation is associated with a higher risk of catheter-related infections, while subclavian vein cannulation carries the least risk.
- In intubated patients, Valsalva or PEEP can increase venous distention and facilitate the procedure.
Clinical updates
- Cosme et al. (Intensive Care Medicine, 2024) analyzed 55,663 central venous catheters from 193 French ICUs (2018–2022) and found low CRBSI rates (<1 per 1000 catheter-days) with no significant difference between internal jugular (0.7), femoral (0.7), and subclavian (0.6 per 1000 catheter-days; adjusted IRR femoral vs IJ 1.04, SC vs IJ 0.82). While subclavian access was associated with significantly lower catheter colonization (IRR 0.54 vs IJ) and femoral access with higher colonization (IRR 1.12), these differences did not translate into differences in CRBSI rates, challenging the traditional hierarchy of insertion sites. Microbiology was dominated by coagulase-negative staphylococci (27.9%), Enterobacterales (27.5%), Candida spp. (16.9%), and S. aureus (16.9%), with more S. aureus in IJ lines and more Candida in subclavian lines.
Cosme V, Massart N, Reizine F, et al. Central venous catheter-related infection: does insertion site still matter? A French multicentric cohort study. Intensive Care Med. 2024;50(11):1830-1840.