Goal
Rule in severe valvular disease of the tricuspid, mitral, and aortic valves.
It is important to stress that POCUS should never replace official transthoracic echocardiography, and an official advanced echocardiographic assessment is required for incidental or abnormal findings.
Most common causes of valvular pathology:
- Endocarditis: Bacteremia or fungemia
- Valve stenosis: Calcification, congenital disorder
Valve regurgitation: Ischemia, chronic hypertension, congenital disorder
Views
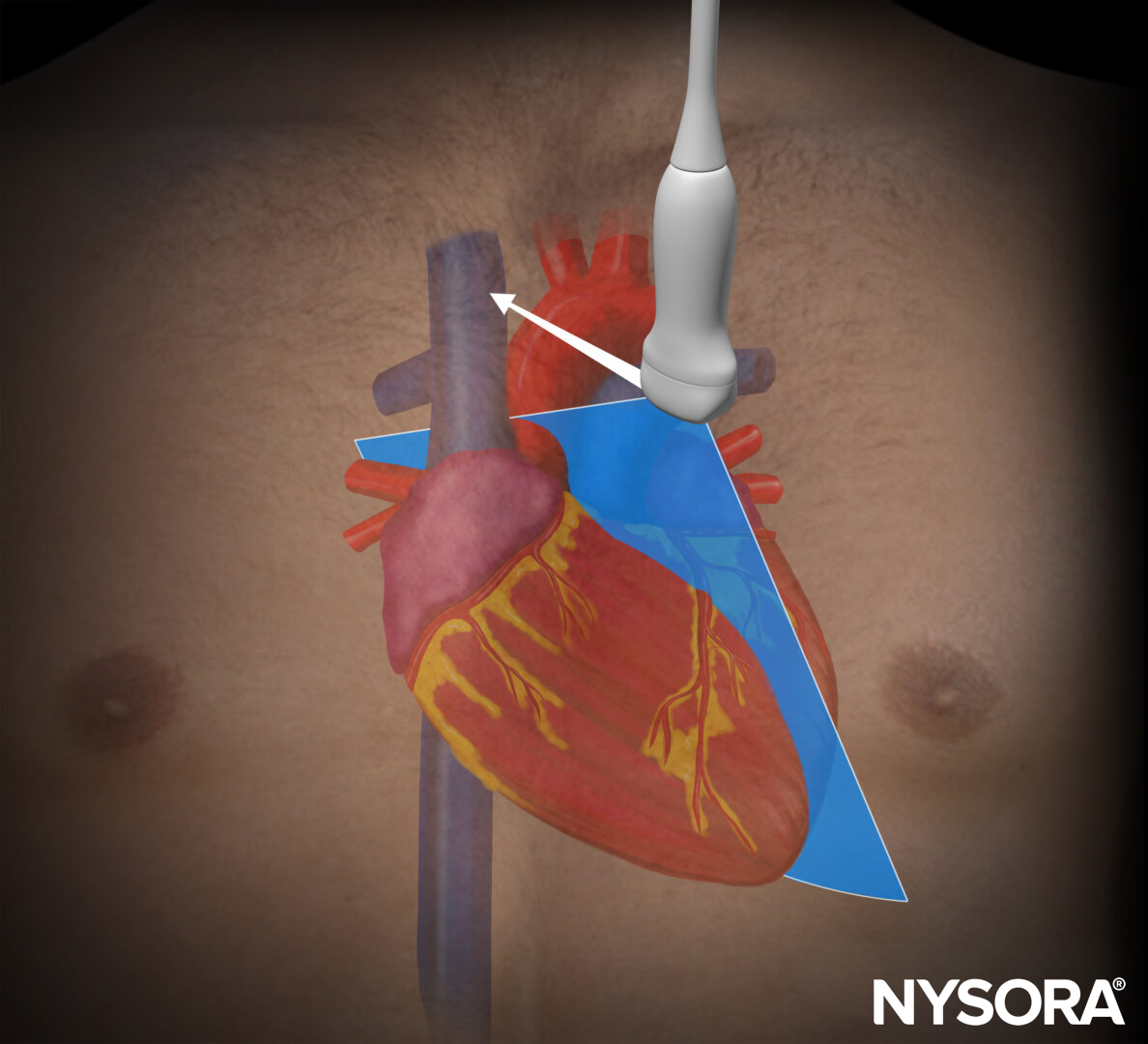
Parasternal long-axis view (PLAX): mitral and aortic valves

Transducer position and sonoanatomy of the parasternal long-axis view.
Parasternal short-axis view (PSAX): mitral and aortic valves
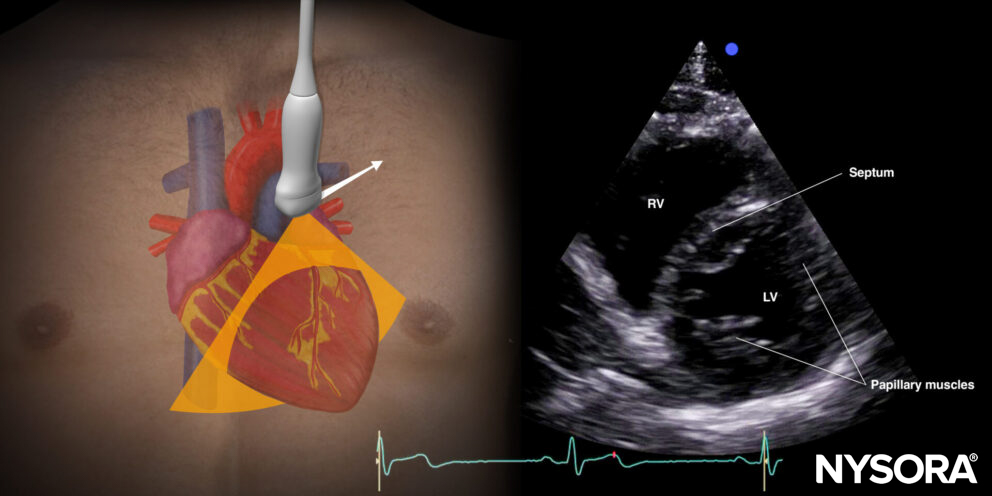
Transducer position and sonoanatomy of the parasternal short-axis view.
Apical four-chamber view (A4C): tricuspid, mitral, and aortic valves
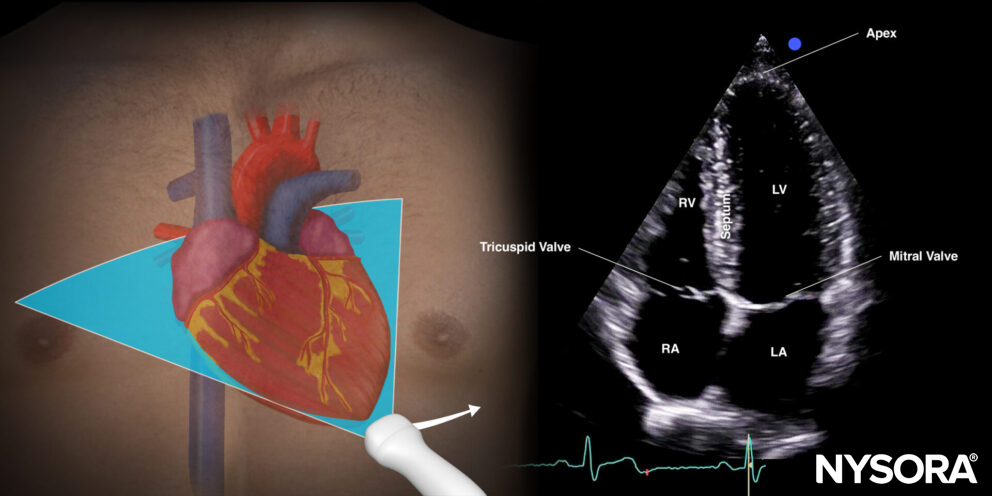
Transducer position and sonoanatomy of the apical four-chamber view.
Assessment
Valvular assessment requires 2D ultrasound and color Doppler:
- 2D ultrasound of the valve: assess calcification (hyperechogenic), leaflet mobility, thickening, mass, or lesion.
- Color Doppler: assess flow or jet area, turbulence (aliasing).
- Categorize whether the finding is severe or not.
Pathology characteristics
- Endocarditis
- Mobile lesion
- Hyperechoic density
- Endocarditis is often accompanied by regurgitation
- Stenosis
- Thickened valve leaflets
- Stiff or minimal movements of the leaflets
- Small valve opening
- A cardiac murmur with a normal aortic valve on ultrasound rules out severe aortic stenosis
- Regurgitation
- Color Doppler: When blood velocity exceeds the Nyquist limit, aliasing occurs. This is a turbulent flow that appears as multicolored blood flow. Aliasing with large jets is typical for regurgitation.
- The mitral or tricuspid valve regurgitation is severe if the jet occupies more than 50% of the atrium or hits the back wall of the atrium.
- The aortic regurgitation is severe if the jet over the aortic valve occupies the majority (65%) of the left ventricle outflow tract.
- Jets that are not seen at the center of the valve are often underestimated and should be considered severe until proven otherwise.
Tips
- Always consider the hemodynamic impact and the clinical context.
- Reduce artifact burden during endocarditis screening by assessing the lesion in multiple planes.
- Valve stenosis may be accompanied by other findings, such as myocardial hypertrophy or atrial enlargement.
- The quantification of severe stenosis requires spectral Doppler assessment of the valve.
- Assessment after valvular surgery should be performed by certified sonographers.
Color Doppler tips
- Use a high Nyquist limit (50-70 cm/s) and color gain just below spontaneous speckling for cardiac valve assessment.
- Minimize imaging depth
- Narrow image sector size
- Use the smallest color box that includes the valve and receiving chamber of interest
- Freezing the color Doppler image and scrolling through the clip may improve the visibility of the flow.
- The color box should be large enough to capture both the valve and the area of interest, i.e., atrium/LVOT.
- Suboptimal angles toward the jet may underestimate the size.
Clinical updates
Mizubuti et al. (Canadian Journal of Anesthesia, 2024) defined seven core valve assessment competencies for basic perioperative FoCUS using a national Delphi process, emphasizing recognition of gross (severe/critical) valvular disease rather than quantitative grading. Competencies include identifying severe aortic stenosis (calcified/restricted leaflets, LVH), gross aortic insufficiency (diastolic turbulent colour Doppler), mitral stenosis (thickened/restricted leaflets ± CW Doppler for gradient), mitral regurgitation (LA dilation, systolic colour jet), tricuspid stenosis/regurgitation, and systolic anterior motion of the mitral valve with LVOT obstruction, highlighting qualitative 2D and colour Doppler assessment while reserving advanced quantitative measures beyond basic anesthesiology training.
- Mizubuti GB, Maxwell S, Shatenko S, et al. Competencies for proficiency in basic point-of-care ultrasound in anesthesiology: national expert recommendations using Delphi methodology. Can J Anaesth. 2024;71(7):967-977.