Indications
Bowel POCUS can be used in the setting of acute abdomen, ileus, or when small bower obstruction is suspected.
Functional anatomy
Anatomy of the abdomen
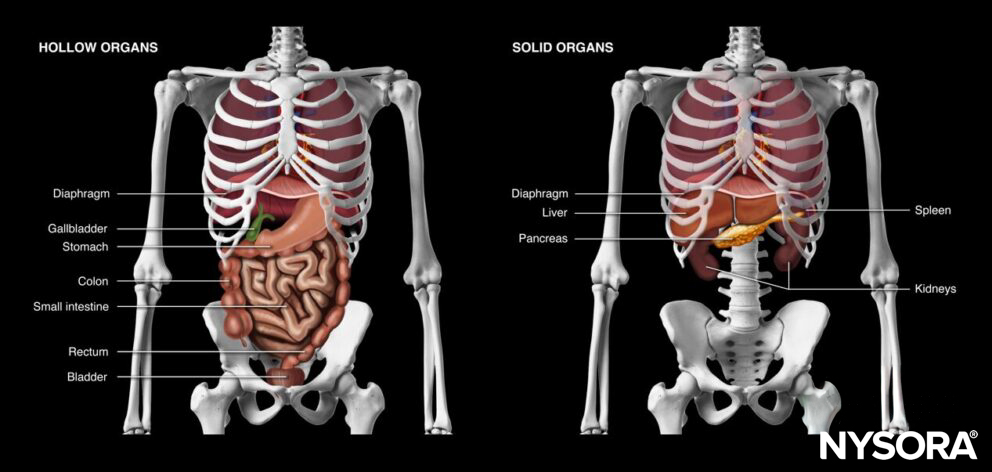
Hollow and solid organs of the abdomen.

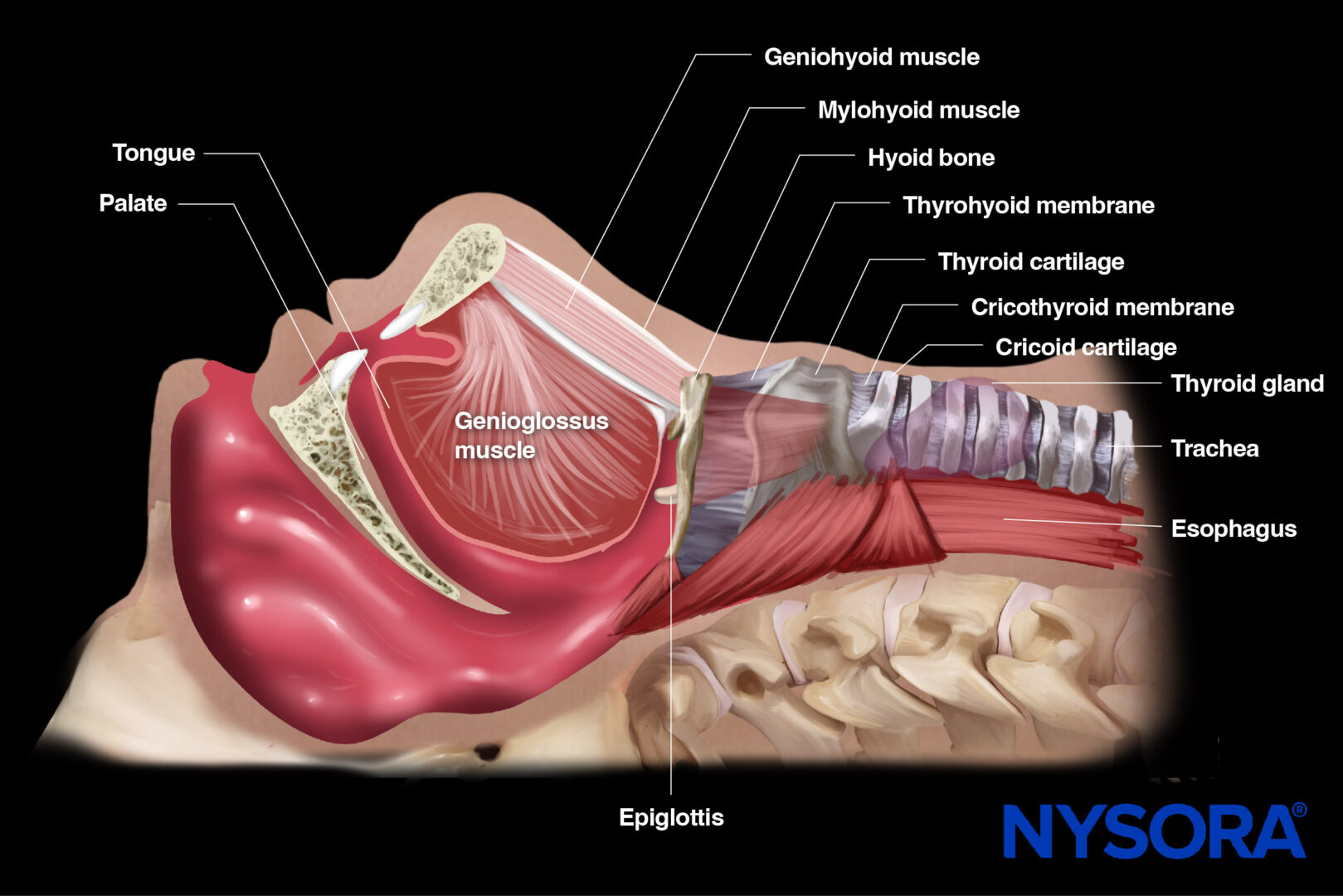
Sagittal section through the abdomen and its relevant anatomy (female).
Anatomy of the bowels
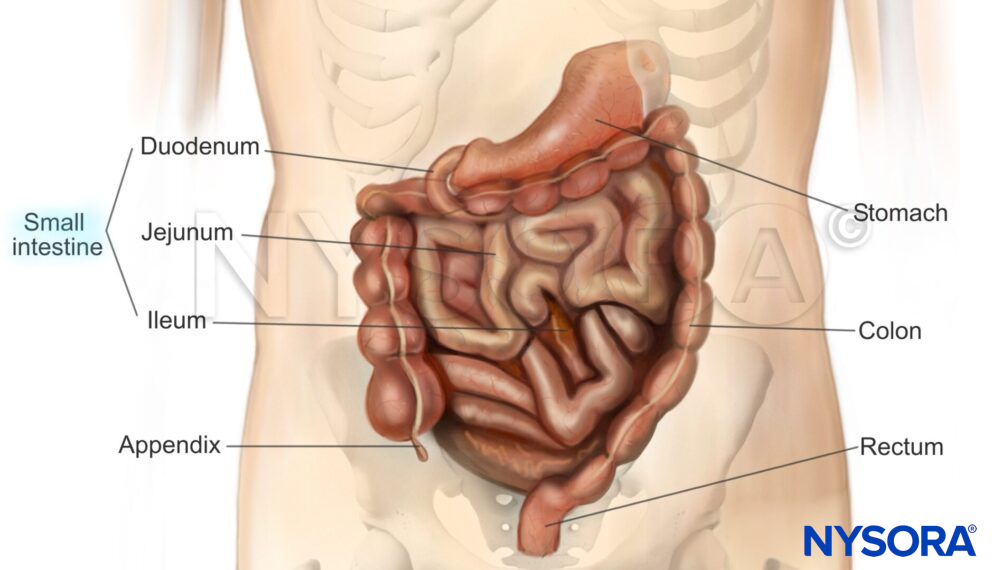
Anatomy of the bowels.
Ultrasound machine setup
- Transducer: curvilinear (or a linear transducer in children or slim adults)
- Ultrasound preset: abdominal
- Orientation: index mark towards the right side of the patient
- Depth: 5 – 10 cm
Patient position
Position the patient supine and completely flat, with the arms abducted.

Patient position for bowel ultrasound.
Landmarks
- Costal margin: ribs in the upper abdomen protect the upper abdominal organs but may limit the acoustic window to the liver, spleen, and kidneys
- Xiphoid process: the upper border of the abdomen
- Linea alba: midline of the abdomen that separates the rectus abdominis muscles and connects the xiphoid process with the pubic bone.
- Umbilicus: virtually separates the abdomen into four quadrants
- Pubic bone: a bony structure and the lower margin of the abdomen. The pelvis starts at the level of the pubic bone.
Anterior superior iliac spine: a bony structure that forms the lateral border of the pelvis
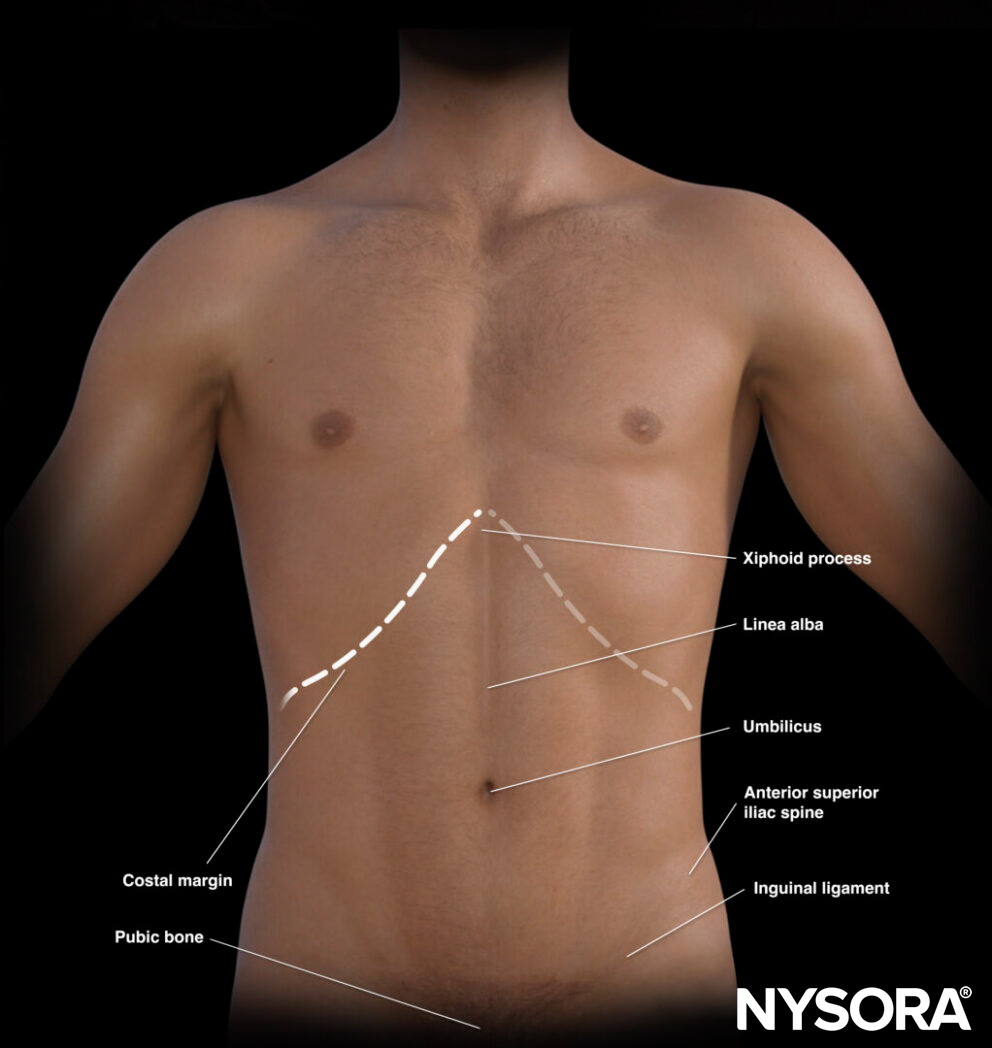
External landmarks of the abdomen.
The umbilicus divides the abdomen into different quadrants that allocate different organs.
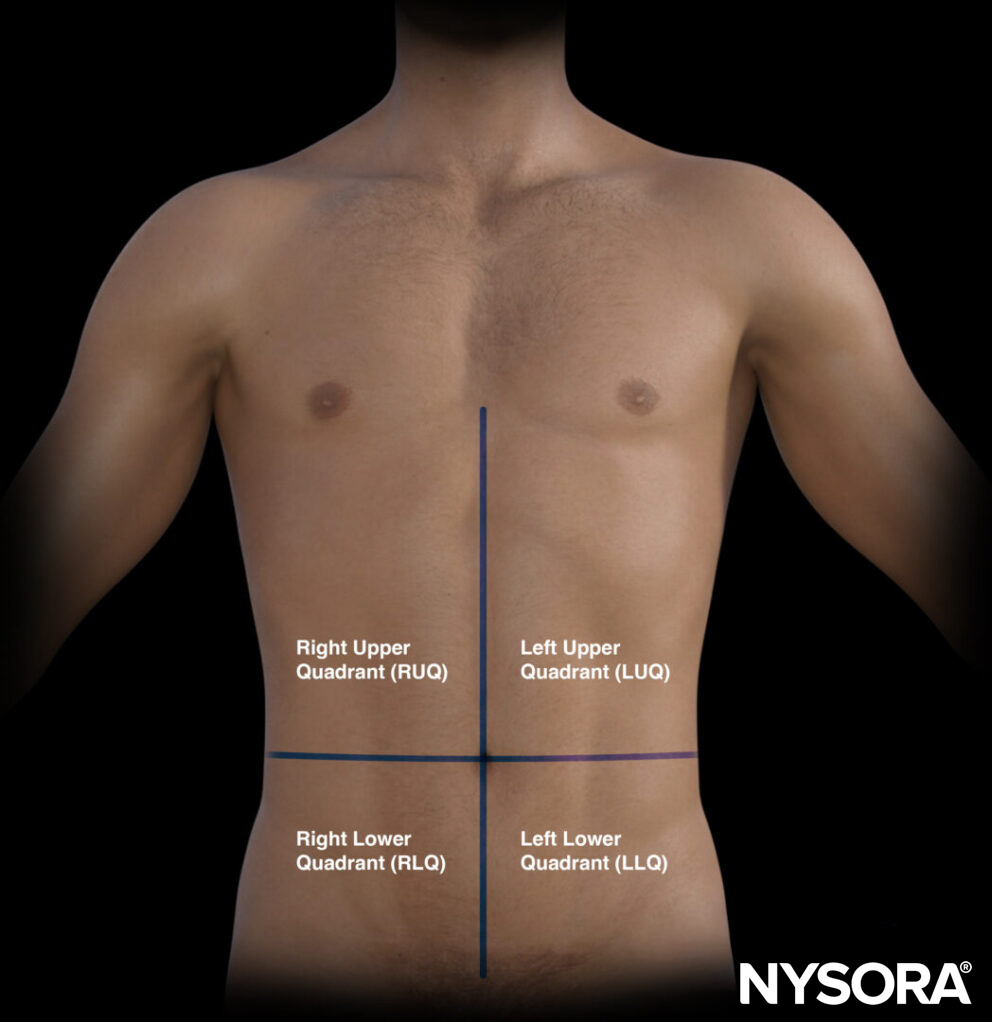
The quadrants of the abdomen.
- Right upper quadrant (RUQ): Liver, gallbladder, kidney
- Left upper quadrant (LUQ): Stomach, spleen, kidney
- Pelvic/paracolic region (lower quadrants): Colon, small intestines, rectum, bladder, male or female reproductive organs
Transducer position
Position the transducer in the RLQ with a transverse orientation and prepare for scanning all four quadrants.
Transducer position for bowel ultrasound.
Scanning
The bowel exam is a dynamic scan. The systematic approach involves hovering the ultrasound transducer over all four quadrants and is described as the ‘mowing-the-lawn’ technique.
‘Mowing-the-lawn’ technique: systematic approach to scanning the abdomen.
In healthy patients, you will not see the full bowel, as the bowel often contains gas, which results in an acoustic shadow that obliterates the view of deeper structures.
It is, however, possible to assess the bowels for:
- Peristalsis
- Small bowel obstruction
Tip
Applying pressure may improve the imaging in the presence of bowel gas.
Peristalsis
The bowel wall near the transducer will not be obscured by bowel gas, allowing peristalsis to be evaluated.
Peristalsis is the normal presence of autonomous wave-like muscle contractions that originate in the wall of the bowels and that move bowel content forward in the digestive tract.
Small bowel obstruction
Specific ultrasound findings are related to small bowel obstruction:
- Dilated bowel loops ( > 2.5 cm)
- The length of the small bowel segment is > 10 cm
- Ineffective or absent peristalsis is imaged by the whirling motion of the bowel contents (‘to and fro motion’)
- Thickened bowel wall ( > 2 mm)
- Collapsed colonic lumen
- Non-compressible small bowel
Tips
- The prominence of the plicae circulares in small bowel obstruction, typically seen in the jejunum, is referred to as the ‘piano’ or ‘keyboard sign’.
- The small bowel sonographically differs from the large bowel by the presence of these plicae circulares.
- The presence of 2 of 3 of the following findings has a sensitivity of 97.7% and specificity of 92.7% for small bowel obstruction: bowel loops > 3 cm, whirling of the intraluminal contents, or collapsed colonic lumen.
- The tanga sign represents the presence of intraperitoneal fluid between the bowels.
- It is not possible to differentiate small bowel obstruction from ileus.
Clinical updates
Abramson et al. (Diagnostics, 2025) propose a two-phase GI POCUS protocol integrating a “lawnmower” anterior abdominal sweep to assess small bowel diameter and peristalsis (normal ≤2.5 cm; ≥2.75 cm abnormal) with targeted gastric evaluation (subxiphoid antrum and LUQ body/fundus) to triage ileus, small bowel obstruction (SBO), gastric dilation, and pneumoperitoneum. They distinguish SBO from ileus by concurrent visualization of dilated (≥2.75 cm) and decompressed small bowel loops, and highlight sonographic detection of free intraperitoneal air within fluid as highly suggestive of perforation. The authors emphasize serial bedside reassessment to monitor the evolution of obstruction and suggest future integration of AI tools to improve acquisition and interpretation in resource-limited settings.
- Abramson L, Theophanous RG, Lefler B, et al. Echoes from Within: Mapping Gastrointestinal Obstruction with Ultrasound. Diagnostics (Basel). 2025;15(19):2511.