Indications
- Emergency surgery
- Non-compliance with fasting instructions
- Unreliable anamnesis: cognitive impairment, children, language barrier, altered sensorium
- Delayed gastric emptying: pregnancy, diabetes, severe liver/kidney dysfunction, critical illness, severe obesity
Quick facts
- Gastric content assessment by ultrasound is unreliable in patients with abnormal gastric anatomy or prior gastric surgery (e.g., hiatus hernia, gastric banding, gastric bypass, gastric sleeve, fundoplication, … ).
- The antrum is usually more superficial than expected (3-4cm)
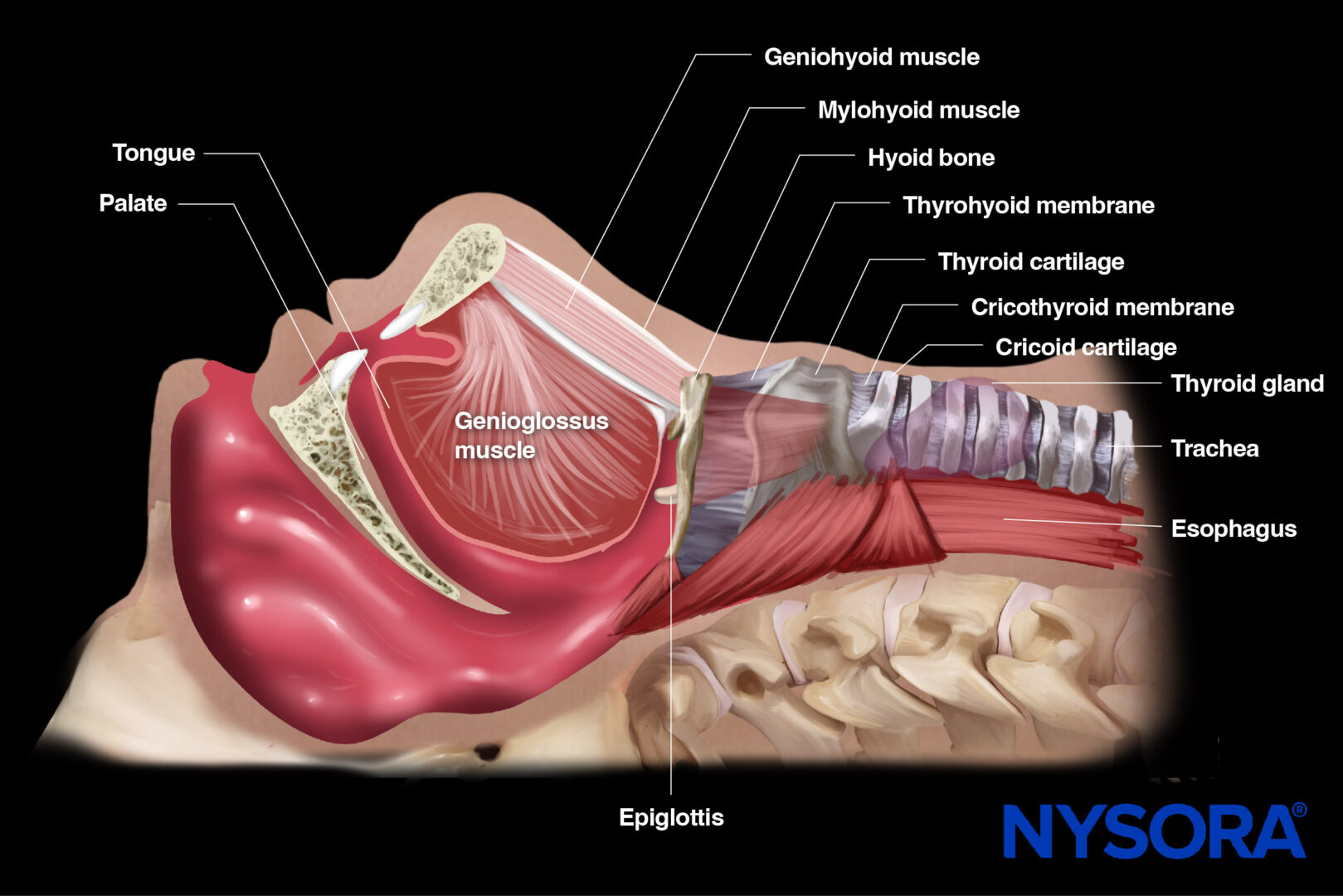
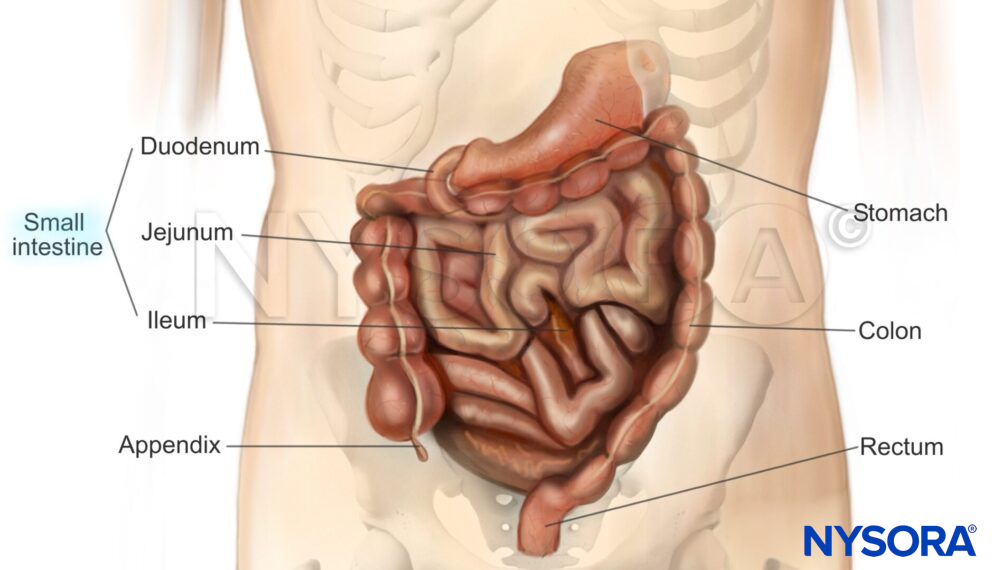
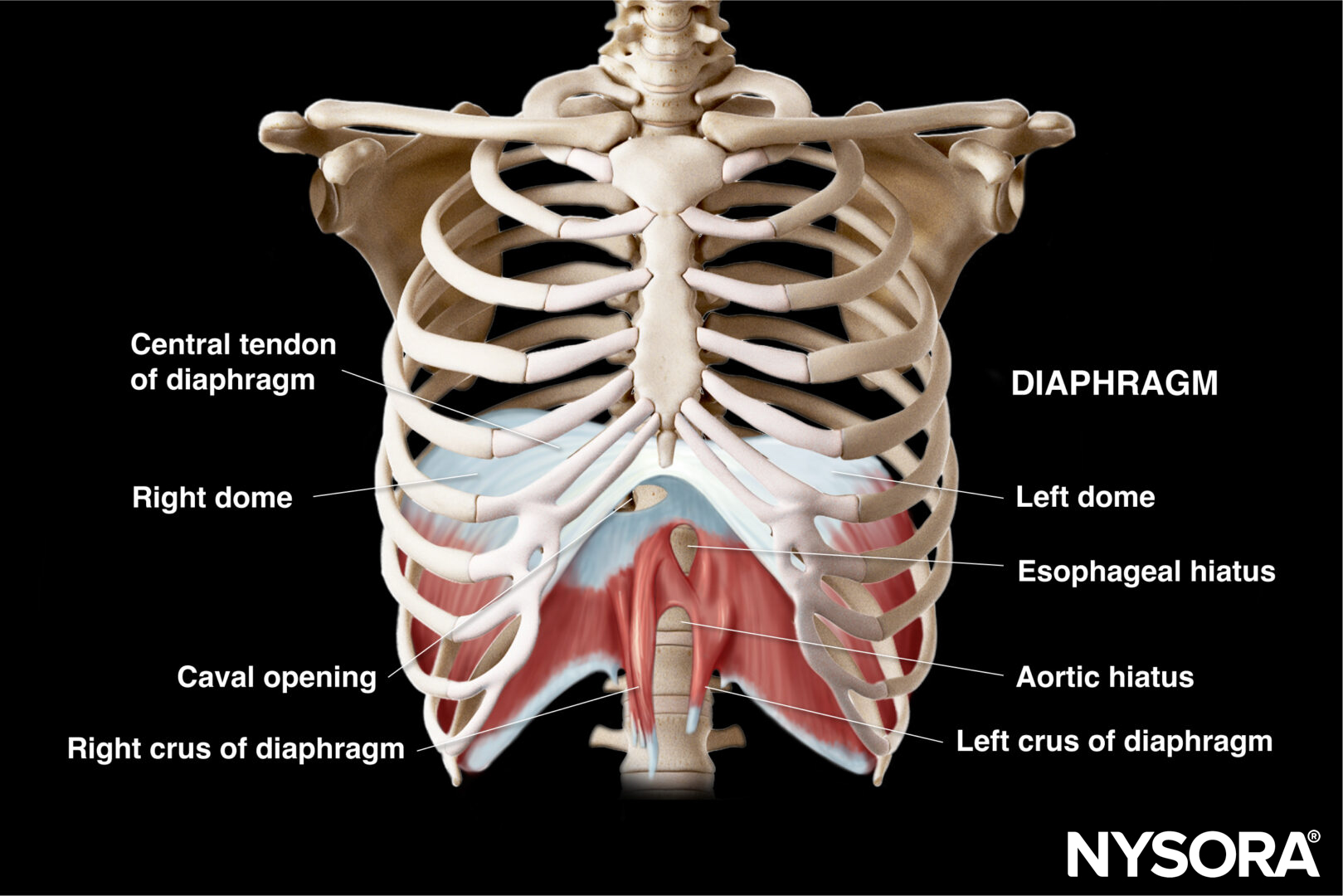
Functional anatomy
Anatomy of the abdomen
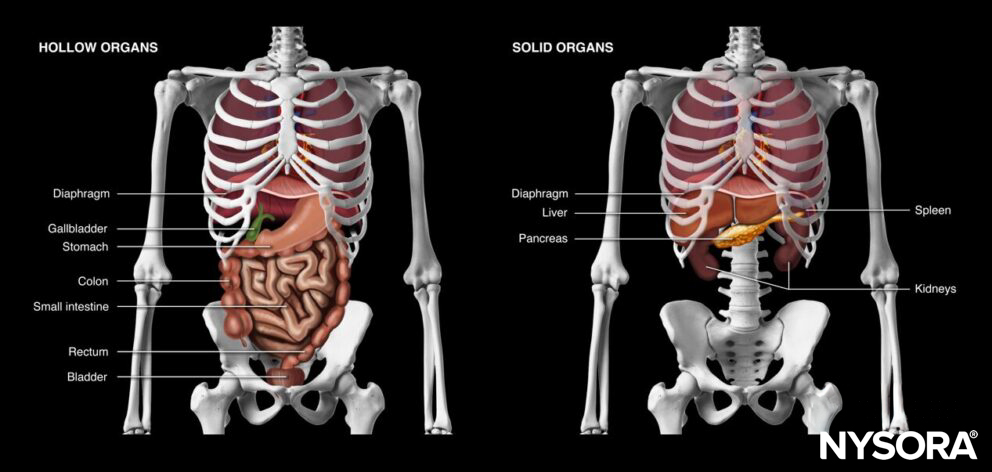
Hollow and solid organs of the abdomen.
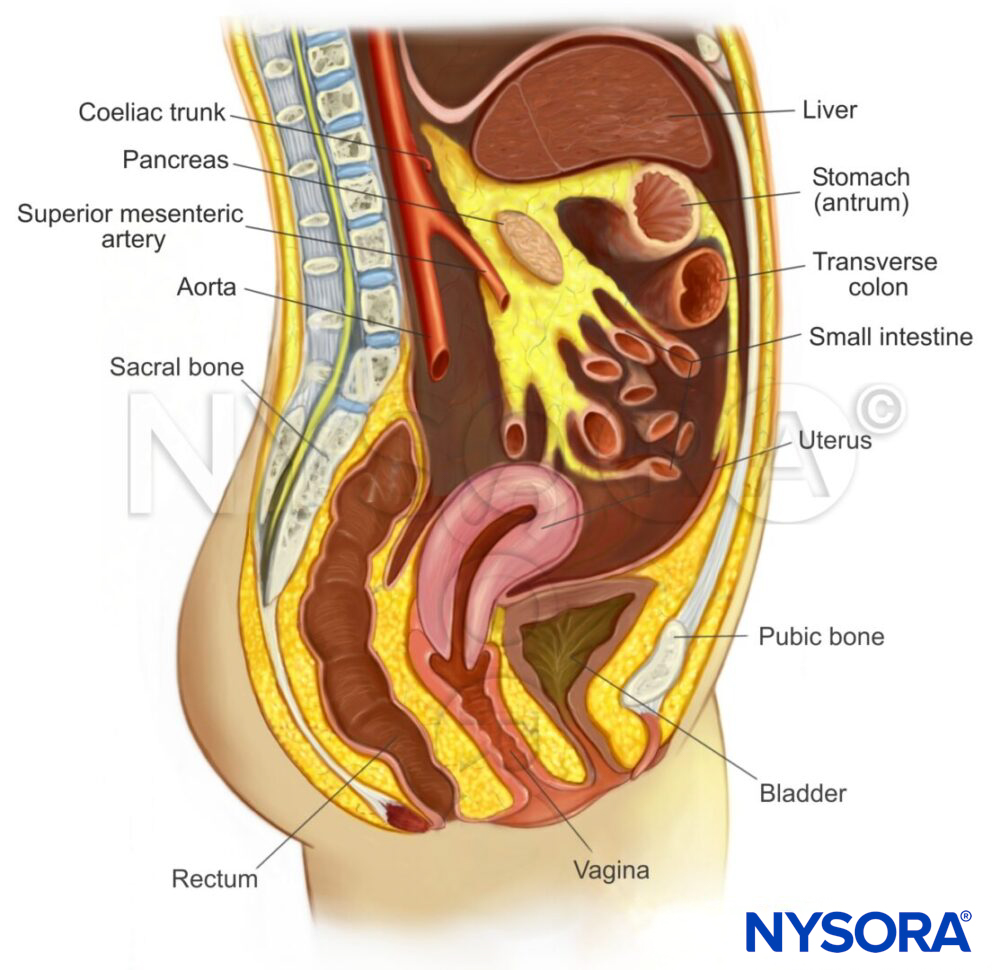
Sagittal section through the abdomen and its relevant anatomy.
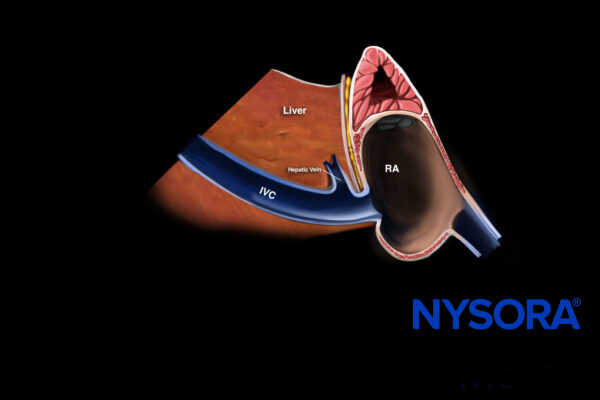
Anatomy of the stomach
The aim of a gastric ultrasound is to obtain a sagittal section through the antrum of the stomach together with the left lower liver lobe, the pancreas, and the aorta. The antrum has a typical round-shaped structure. It is positioned between the liver and the pancreas, it has a multilayered wall, and reflects the content of the entire stomach since it functions as a funnel where the content will collect due to gravity.

Relevant anatomy of the stomach and the surrounding organs.
The structural sonoanatomical pattern of the wall of the stomach consists of four layers, which help to differentiate the antrum from other hollow viscus organs. The most recognizable layer is the hypoechogenic muscularis propria. On the outside of this layer, the serosa can be found, and on the inside, the submucosa and the muscularis mucosa.

The antrum of the stomach with its layers.
Ultrasound machine setup
- Transducer: curvilinear
- Ultrasound preset: abdominal
- Orientation: index mark towards the head of the patient
- Depth: 10 – 15 cm
Tip
For children or adults with a body weight smaller than 30 kg, a linear transducer can be used.
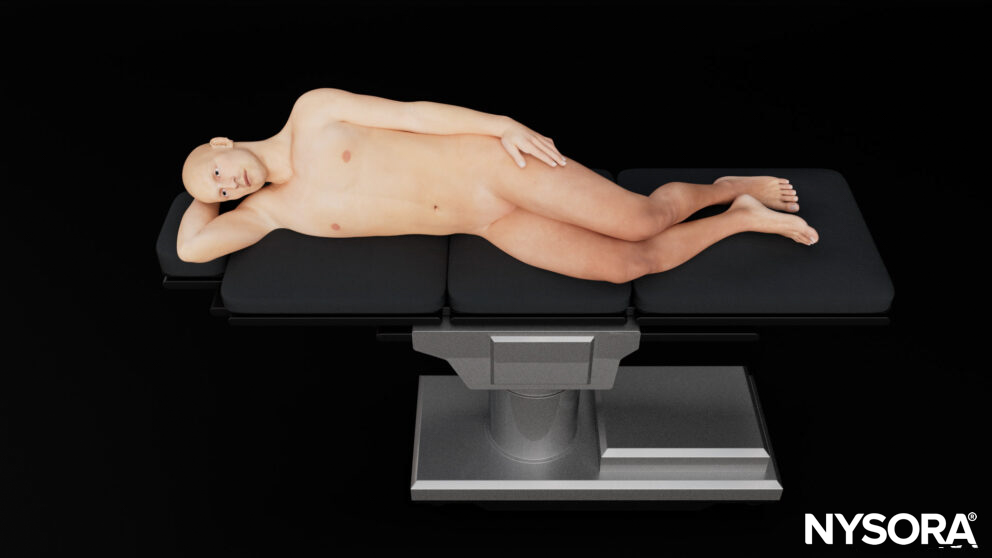
Patient position
In the supine position, large gastric volumes can be visualized in the antrum, but smaller gastric volumes may be displaced to the fundus and may not be visible in the antrum. Therefore, the supine position rules in, but does not rule out a full stomach.

Supine position.
To increase the sensitivity of the examination and rule out a full stomach, the patient is then turned into the right lateral decubitus position.
Right lateral decubitus position.
Tip
Always assess the stomach in the right lateral decubitus position before concluding an empty stomach.
Landmarks
- Costal margin: ribs in the upper abdomen protect the upper abdominal organs but may limit the acoustic window to the liver, spleen, and kidneys
- Xiphoid process: the upper border of the abdomen
- Linea alba: midline of the abdomen that separates the rectus abdominis muscles and connects the xiphoid process with the pubic bone.
- Umbilicus: virtually separates the abdomen into four quadrants
- Pubic bone: a bony structure and the lower margin of the abdomen. The pelvis starts at the level of the pubic bone.

External landmarks of the abdomen.
The umbilicus divides the abdomen into different quadrants that allocate different organs.
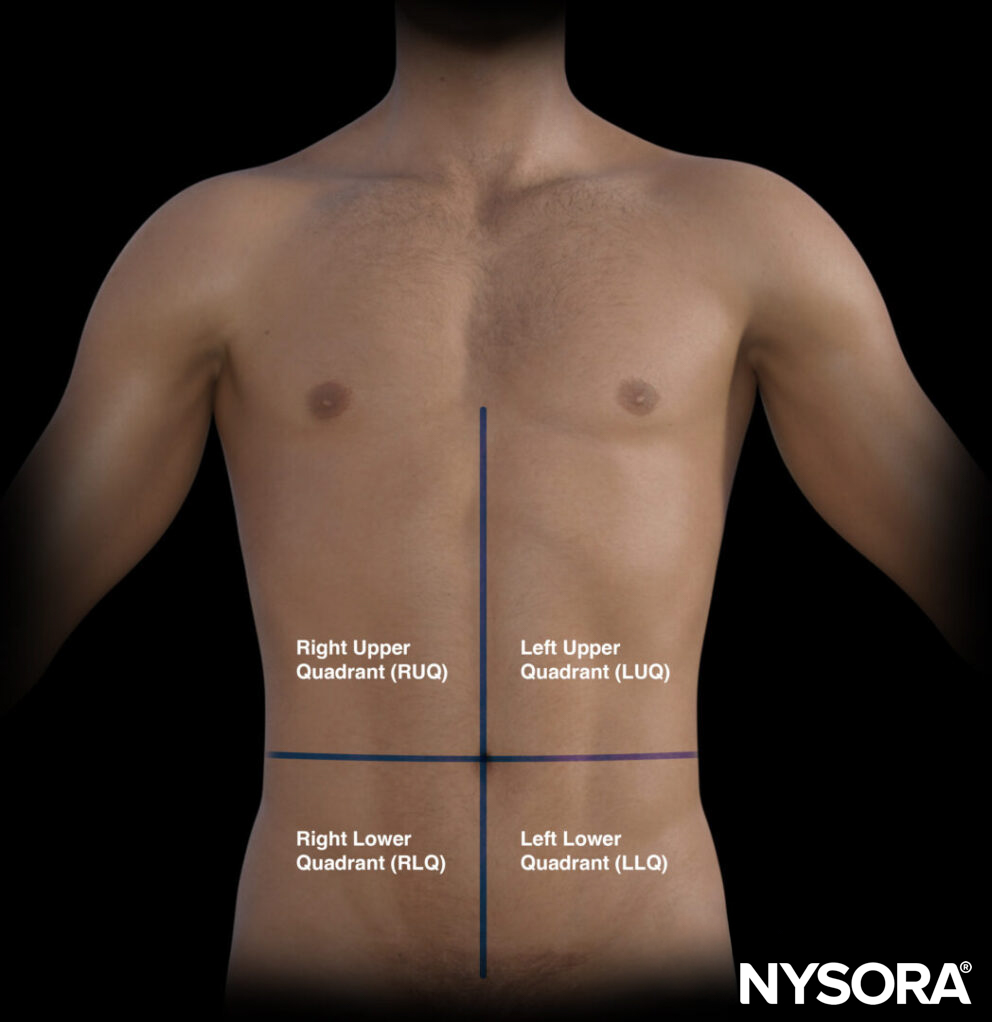
The different quadrants of the abdomen.
- Right upper quadrant (RUQ): Liver, gallbladder, kidney
- Left upper quadrant (LUQ): Stomach, spleen, kidney
- Pelvic/paracolic region (lower quadrants): Colon, small intestines, rectum, bladder, male or female reproductive organs
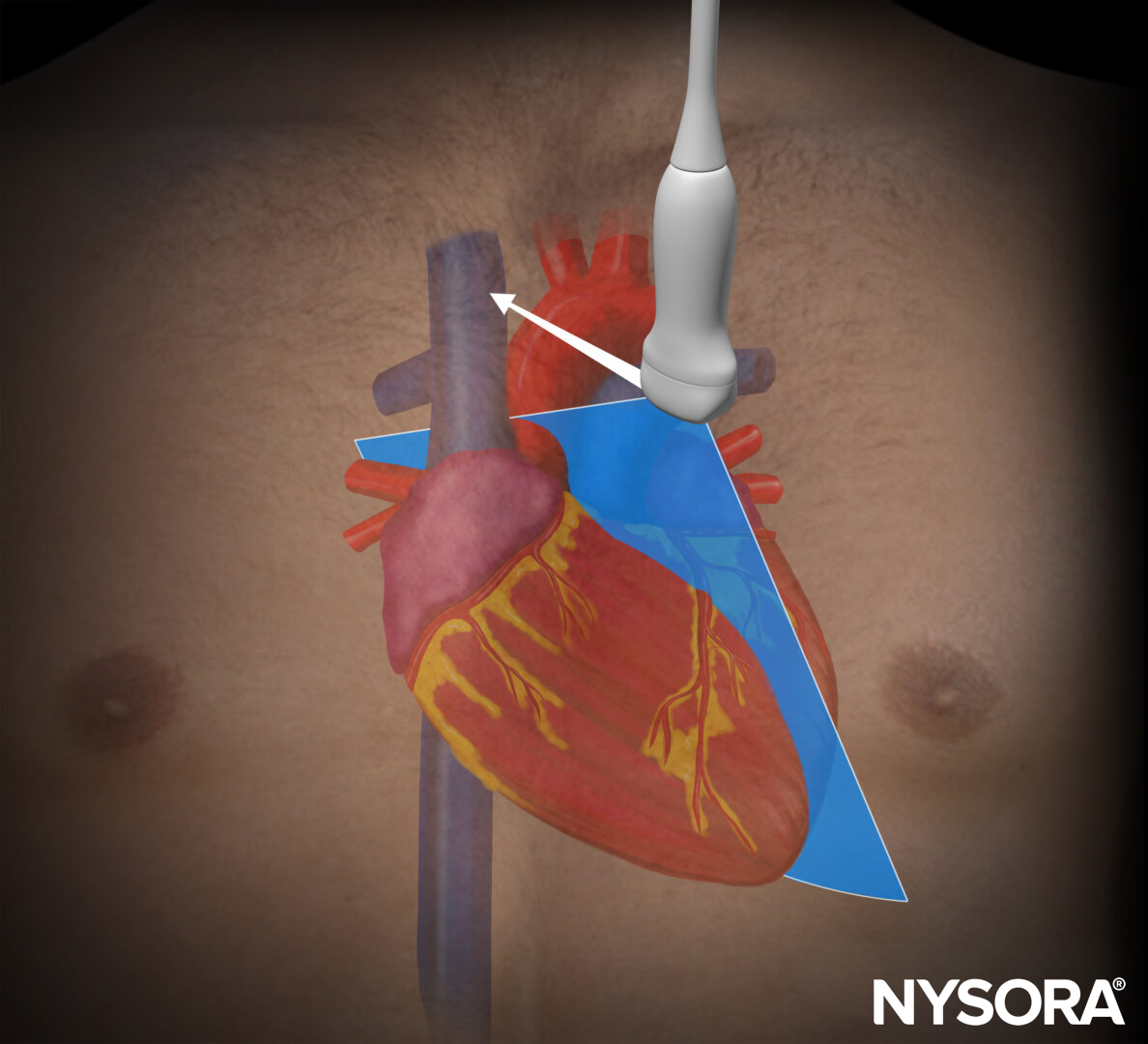
Transducer position
The transducer is positioned underneath the xiphoid and on the midline or linea alba. Then scan caudally until you see the caudal border of the liver and the aorta in the deeper field. Identifying these will make sure you are on the midline and at the level of the antrum.
Transducer position for gastric content assessment.
Tip
Use the liver as an acoustic window.
Scanning
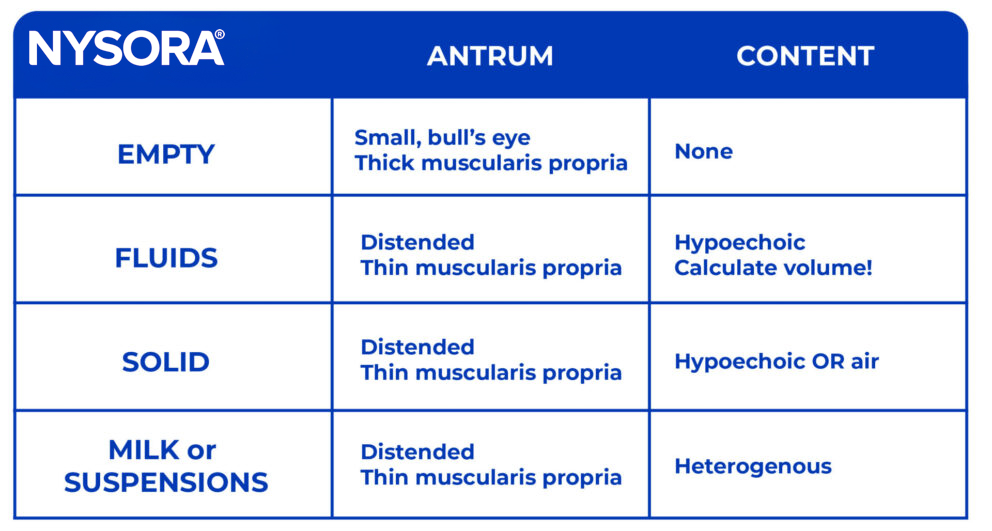
The assessment of gastric content will indicate whether the stomach is empty or filled with fluid or solid material.
Empty stomach
In case of an empty stomach, the antrum has a typical round-shaped or elliptical structure which is often referred to as the bull’s eye pattern. The structural pattern differentiates itself from other structures by a thick hypoechogenic wall built out of muscularis propria with central and external hyperechoic layers, the mucosa, and serosa.
Ultrasound and Reverse Ultrasound Anatomy of an empty stomach.
Fluid content
The presence of intraluminal fluid will result in a rounded and distended appearance of the antrum and thin stomach walls. Sonographically, a differentiation can be made between clear fluids and non-clear fluids (e.g., suspensions or milk). Clear fluids are anechoic, whereas non-clear fluids are hyperechoic.

Ultrasound and Reverse Ultrasound Anatomy of a stomach with fluid content.
Tip
The ingestion of carbonated fluids may result in a transient image with bubbles, also known as the ‘starry night’ appearance.
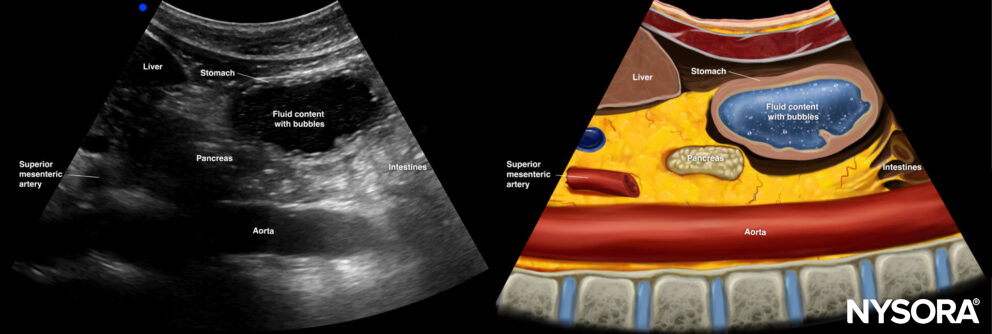
The ingestion of carbonated fluids may result in a transient image with bubbles, also known as the ‘starry night’ appearance.
Solid content: Early phase
In the early phase after intake of solids, solid content is usually mixed with air, resulting in reflection of all the ultrasound beams, making it impossible to visualize the underlying structures. Mixed air and solid content is often described as the ‘frosted glass’ pattern. The wall of the antrum will be thin.
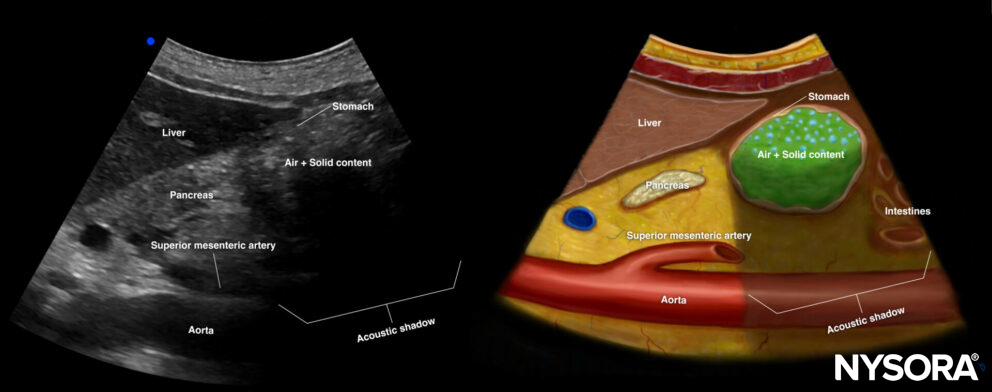
Ultrasound and Reverse Ultrasound Anatomy of a stomach with solid content in the early phase.
Solid content: Late phase
After a couple of hours, the air will disappear, and the content will be better outlined as gastric content with a mixed echogenicity.
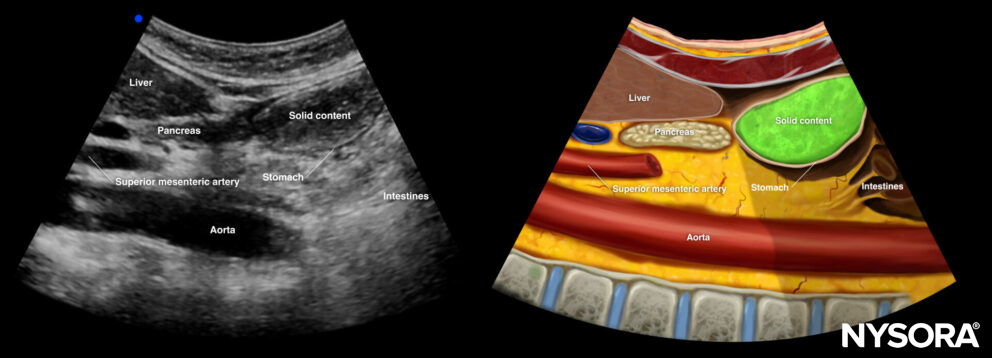
Ultrasound and Reverse Ultrasound Anatomy of a stomach with solid content in the late phase.
Interpretation
Step 1: Define the content in the supine position
Overview of stomach content grading.
- If solid content is present, there is a high risk of aspiration.
- An empty stomach or fluid content requires further imaging in the right lateral decubitus position.
Step 2: Define the content in the right lateral decubitus position.
- If no content is seen in the right lateral decubitus position, the stomach is empty (grade 0).
- If fluid content is visualized in the right lateral decubitus position, measure the cross-sectional area (CSA) by tracing the outer layer of the antrum or the serosa.
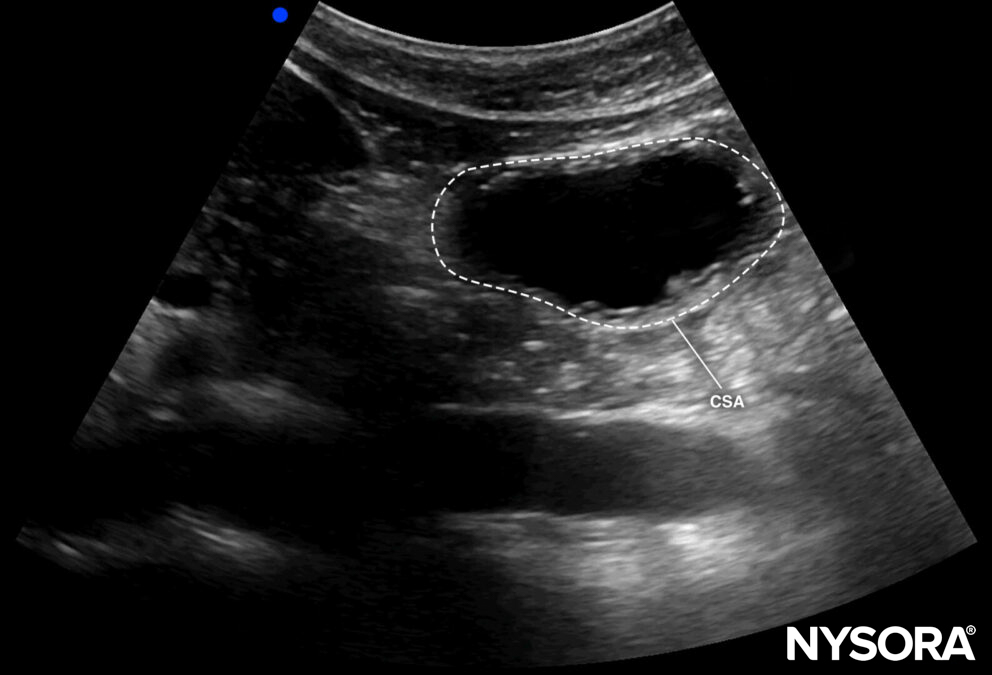
Cross-sectional area of the antrum.
- By using the CSA and the age of the patient, the volume can be estimated according to the formula:
Gastric volume = 27.0 + (14.6) x (CSA of antrum in right lateral decubitus position) – 1.28 x age
- If the fluid content is >1.5 mL/kg, the stomach is considered at risk for aspiration or full (grade 2).
- A fluid content < 1.5 mL/kg is compatible with a fasting state (grade 1).
Tips
- In case the ultrasound machine does not have a free tracing tool to measure the CSA, the area can be calculated by using two perpendicular diameters and the formula of the area of an ellipse: CSA = (anteroposterior diameter × craniocaudal diameter × π) / 4
- No peristaltic movements should be present during the measurement.
- Quick decision tables are available to determine gastric content based on age and CSA.
Step 3: Decision making
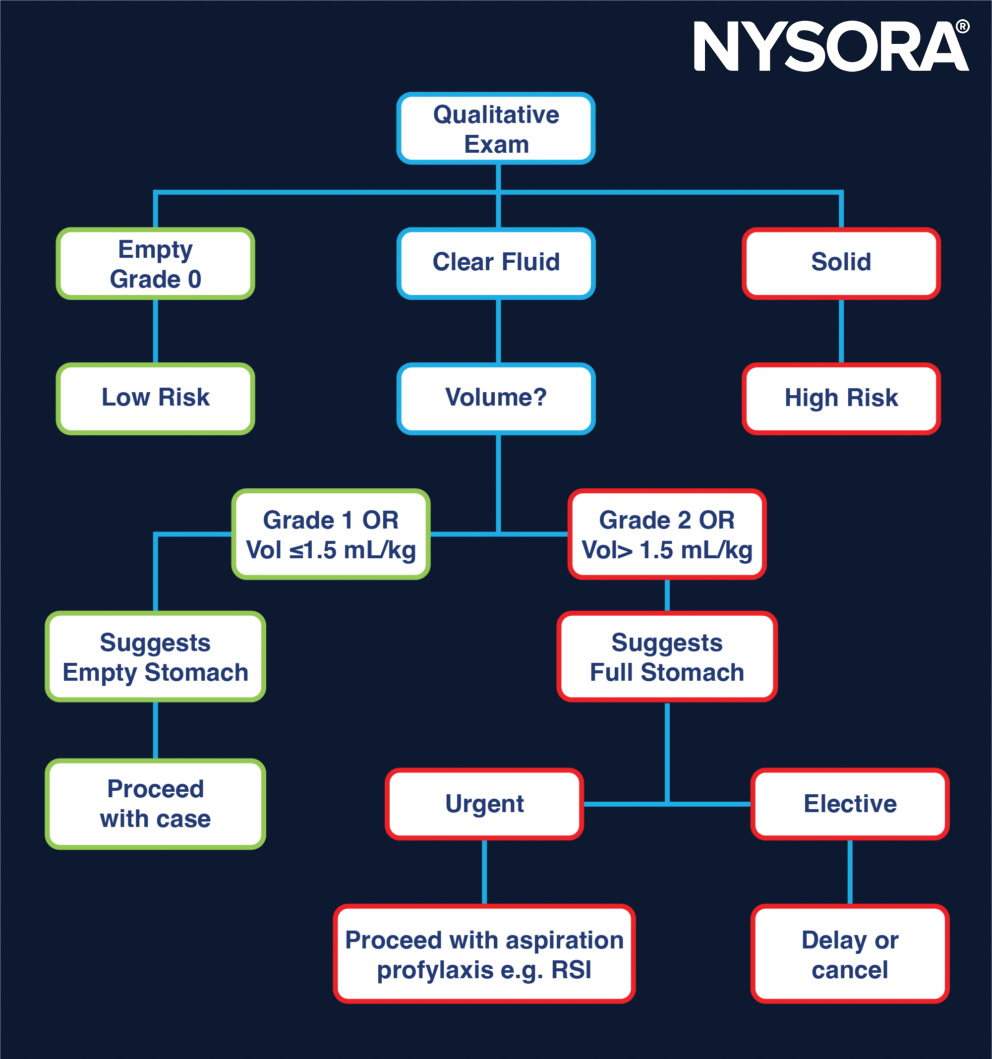
Decision pathway as suggested by Perlas et al.
Overview
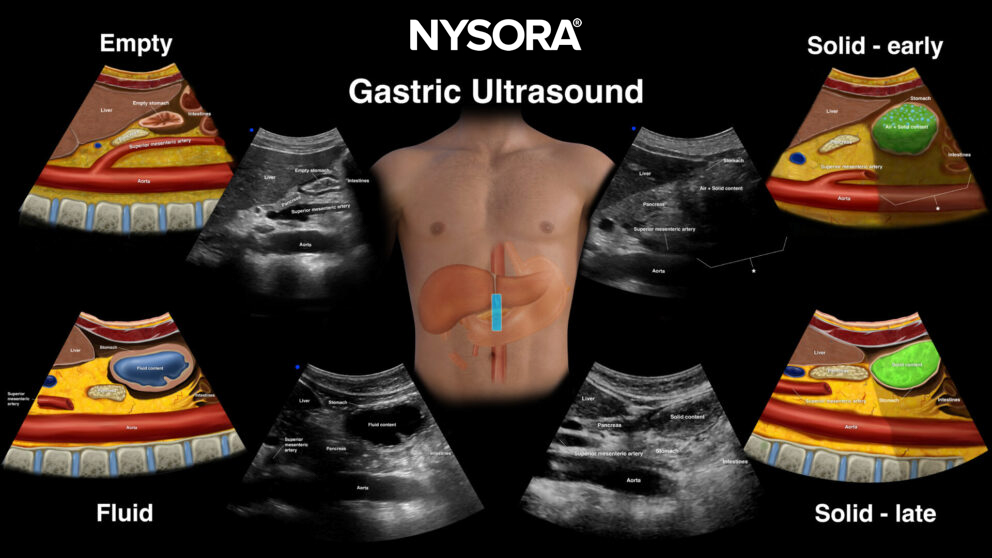
Overview of the different types of gastric content.
Clinical application: anesthesia for emergency surgery
Introduction
The timing of emergency surgery and the technique of anesthesia are challenging in
patients with a history of recent food intake. The presence of gastric content increases the risk of aspiration, potentially resulting in acute lung injury, pneumonia, or death. Delayed gastric emptying complicates the estimation of aspiration risk. Surprisingly, there are no fasting guidelines for emergency surgery. So this is where gastric ultrasound can play a major role.
Fact
Approximately 10% of all surgical procedures involve emergency surgery.
Evidence
Four prospective observational studies reported a 27%-56% incidence of a ‘full stomach’ on gastric ultrasound at the time of induction in the emergency surgery population. These studies also show that there is no correlation between preoperative fasting time and the presence of a full/empty stomach:
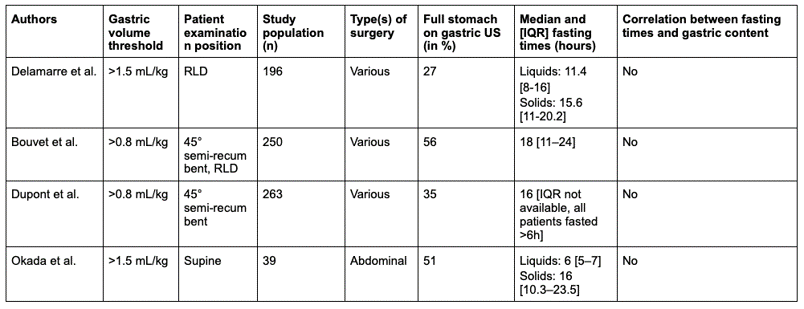
Overview of the available studies investigating the preoperative gastric content in the emergency surgery population by gastric ultrasound with their respective study characterissics. RLD, right lateral decubitus position.
The presence of preoperative gastric content in emergency surgery is high, and the clinical estimation is unreliable. Therefore, a gastric ultrasound can help.
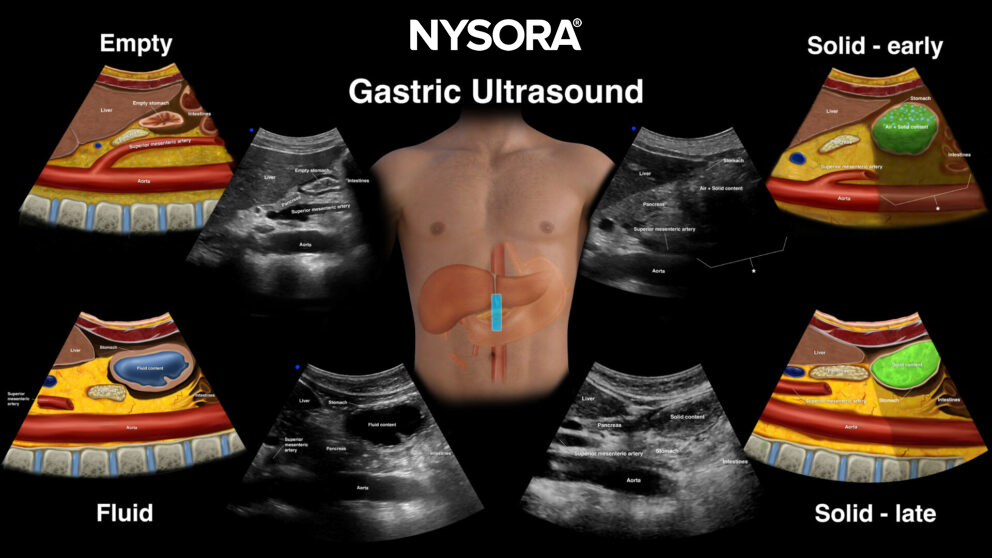
Overview of different types of gastric content that can be visualized with gastric ultrasound
Decision making
Gastric ultrasound should be considered in every case of emergency surgery, but exceptions can be made for high urgency surgery and polytrauma patients, when gastric ultrasound is not feasible, and for patients where the presence of gastric content is certain (absence of clinical relevance).
The following pathway can guide clinical decision-making with gastric ultrasound in emergency surgery patients. It is based on current clinical expert opinion and evidence.

Clinical decision pathway for anesthesia in emergency surgery based on gastric ultrasound.
Fact
In 4 to 14% of cases, it is impossible to acquire a sonographic sagittal image of the antrum, resulting in an inconclusive examination.
Clinical updates
Ruiz Ávila et al. (The Ultrasound Journal, 2023) conducted a prospective correlation study in 41 mechanically ventilated ICU patients receiving enteral nutrition and found good-to-excellent intra- and inter-observer reliability for gastric ultrasound assessment of antral area and gastric volume, with intra-observer CCC 0.94–0.95 and inter-observer CCC 0.84 for both antral area and calculated gastric volume. Qualitative grading showed almost perfect agreement (κ=1.0 supine), and 92% of scans were grade 2 (fluid visible in both positions), with 75% demonstrating gastric volumes >1.5 mL/kg, indicating a high aspiration risk in this population.
- Ruiz Ávila HA, Espinosa Almanza CJ, Fuentes Barreiro CY. Inter-observer and intra-observer variability in ultrasound assessment of gastric content and volume in critically ill patients receiving enteral nutrition.