Goal
POCUS can guide the detection of intravascular high or low volume status by inferior vena cava and lung ultrasound. This can be used to estimate fluid responsiveness.
Etiology
Shock, hypotension, bleeding, postoperative cases with intravascular fluid shifts, cardiac failure, pulmonary hypertension, etc.
Tips
Conditions that increase the right ventricular pressure limit the use of ultrasound of the inferior vena cava and may result in falsely high venous pressures with no respiratory variation:
- Tamponade
- Tricuspid valve regurgitation
- Pulmonary hypertension
- High PEEP
Views
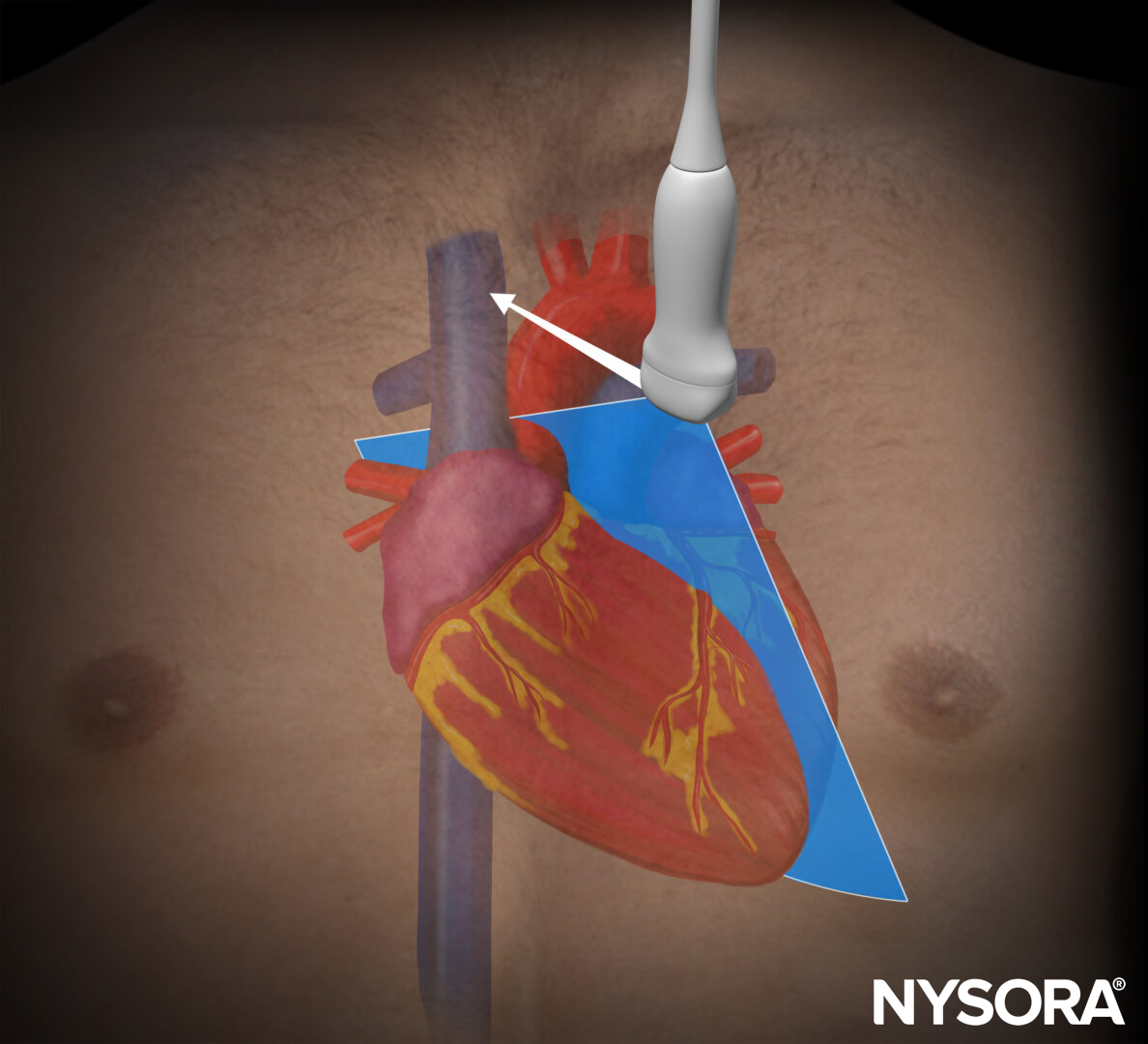
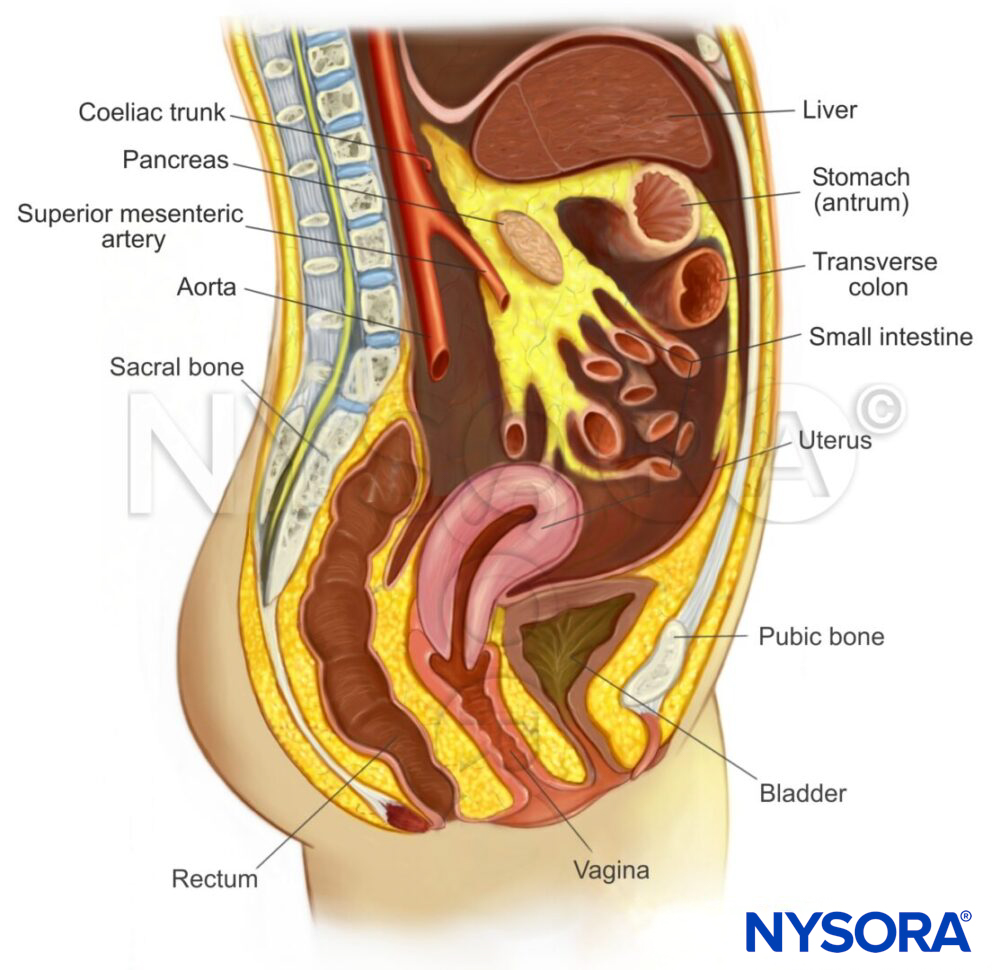
Inferior vena cava view

Transducer position and sonoanatomy of the inferior vena cava view.
A scan of all four BLUE points

BLUE points on the left and right thorax.
Assessment
Inferior vena cava view
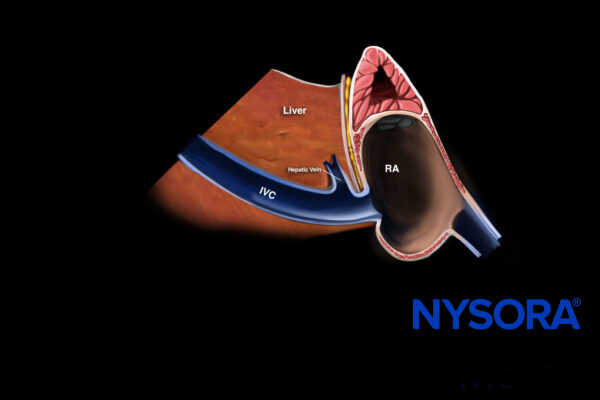
Obtain a view of the inferior vena cava and use M-mode 2 cm distal to its junction with the right atrium or 1 cm distal to the hepatic vein. This will show the respiratory variation in the diameter of the inferior vena cava.
The respiratory variation of the inferior vena cava is indicative of the volume status of the patient and correlates with the central venous pressure and thus the right atrial pressure. This can be used to estimate the volume responsiveness.
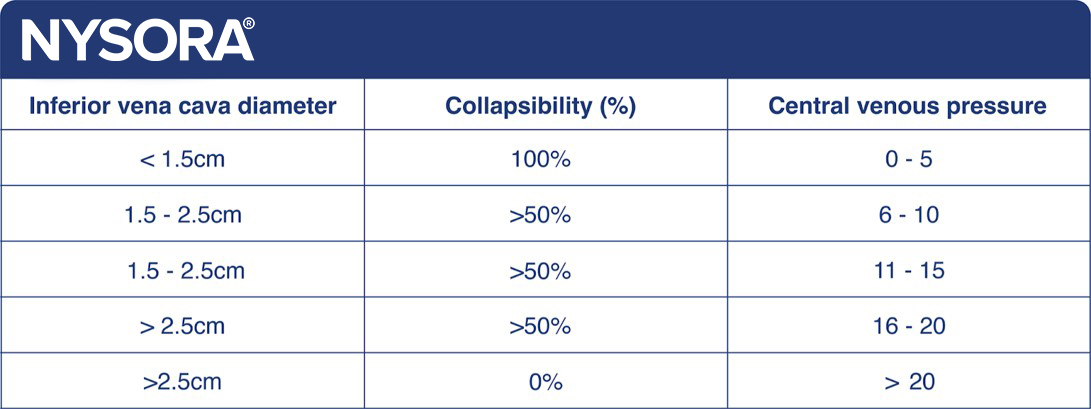
Correlation between IVC diameter, collapsibility, and central venous pressure.
Note
The type of ventilation (spontaneous vs. ventilated) will affect intrathoracic pressure and, in turn, the diameter of the inferior vena cava.
Tip
Do not confuse the inferior vena cava with the aorta. The aorta is surrounded by hyperechoic, fatty tissue, has an angle toward the dorsum of the patient, and is pulsatile.
In spontaneously ventilating, non-intubated patients, the vena cava is minimal during inspiration and maximal during expiration. Patients with a collapsibility index of 100% and an inferior vena cava diameter of less than 1.5 cm are likely to be fluid-responsive.
Collapsibility index = (maximum diameter (Dmax) – minimal diameter (Dmin))/ (maximum diameter (Dmax))

Variation in the diameter of the inferior vena cava.
In mechanically ventilated patients, the inferior vena cava is maximally dilated during inspiration and minimally dilated during expiration. Patients with a distensibility index of 18% are likely to be fluid-responsive.
Distensibility index = (maximum diameter (Dmax) – minimum diameter (Dmin))/ (minimum diameter (Dmin))
Notes
- Tidal volumes need to be 8mL/kg or more.
- Positive end-expiratory pressures need to be 5 cm H2O or less.
Patients who are intubated and breathing spontaneously will have mixed physiology due to the patient’s effort and the ventilator’s work. Here, the diameter of the inferior vena cava is unpredictable.
Lung ultrasound
Next, scan the 4 BLUE points. B-lines represent extravascular lung water, and 3 or more B-lines in all 4 BLUE points (B-profile) are likely to be pulmonary edema.
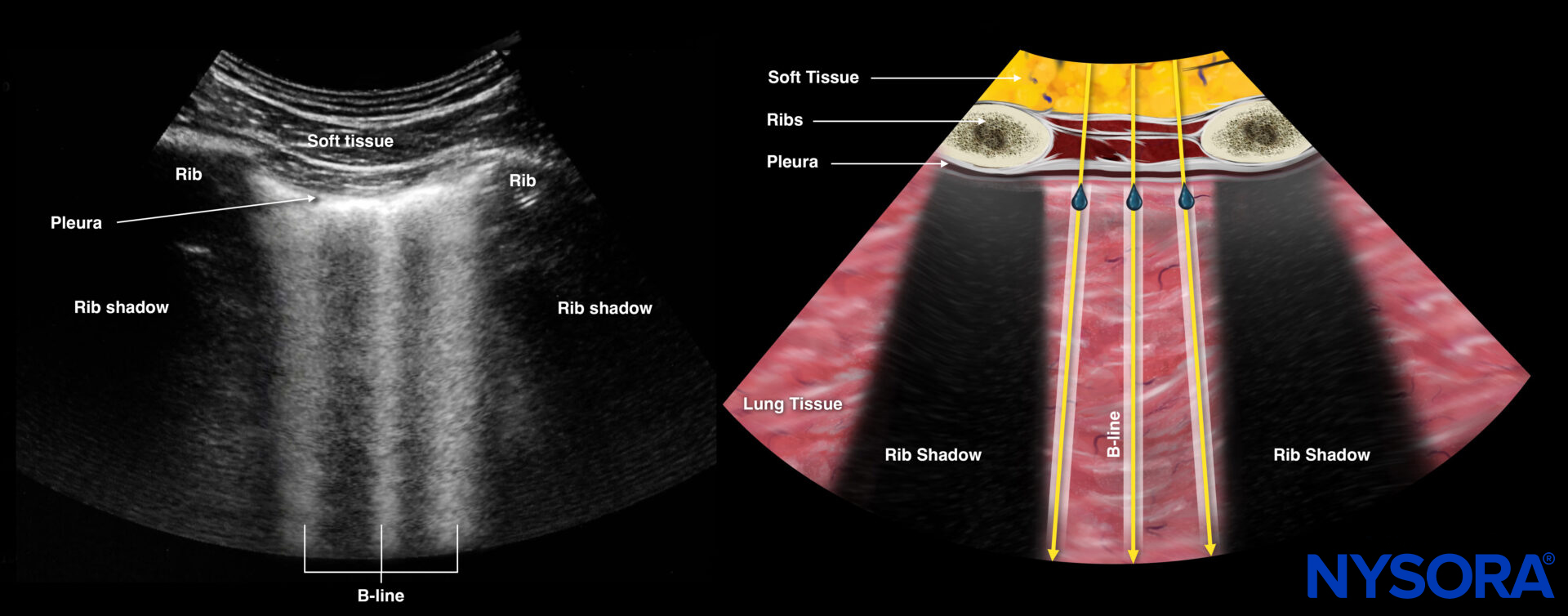
Sonography and Reverse Ultrasound Anatomy of B-lines.
Fluid resuscitation
Ultrasound of the inferior vena cava and the lungs is often used to guide fluid resuscitation. This is a suggested pathway that can be used:
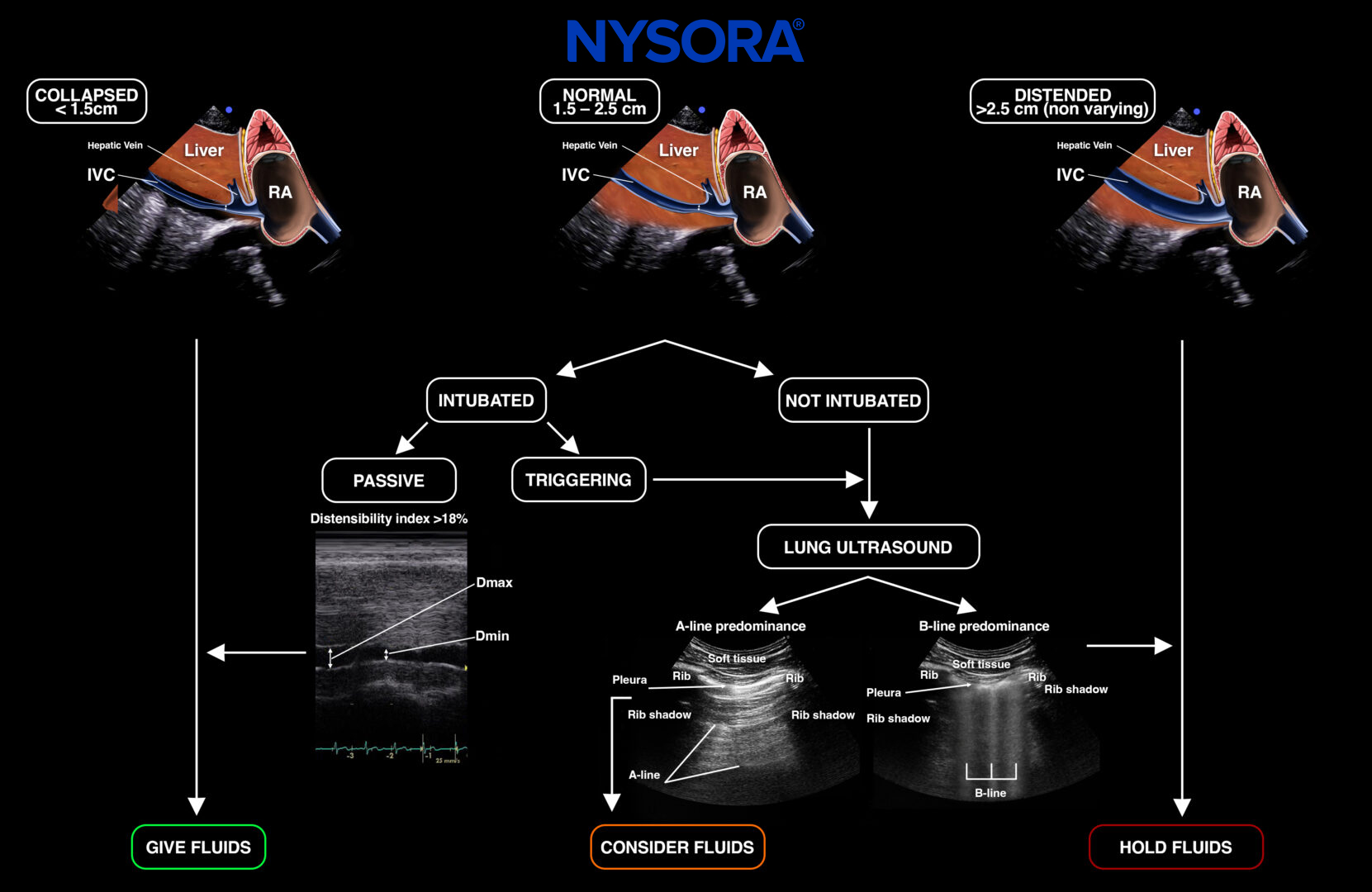
Suggested fluid resuscitation protocol adapted from Lee et al.
Tips
- Respect the limitations of the inferior vena cava assessment.
- Always correlate the clinical image of the patient with ultrasound-guided fluid resuscitation therapy.
Clinical updates
Kan, Arishenkoff, and Wiskar (CHEST, 2025) propose a multiorgan POCUS framework for volume status that integrates five physiologic domains—CVP (IJV/IVC), right heart function, left heart assessment (including LAP and cardiac output via LVOT VTI), extravascular volume (lung B-lines, effusions, ascites, edema), and venous congestion (hepatic, portal, intrarenal Doppler)—to guide fluid responsiveness and fluid tolerance. They emphasize that CVP and IVC findings reflect pressure rather than volume, that elevated LAP or RV dysfunction signals volume intolerance, and that abnormal venous Doppler waveforms identify organ-level congestion even when CVP is normal. The review reframes resuscitation away from targeting forward flow alone (MAP/CO) toward balancing perfusion while avoiding venous congestion, particularly in shock, hypoxia, and AKI.
- Kan JY, Arishenkoff S, Wiskar K. Demystifying Volume Status: An Ultrasound-Guided Physiologic Framework. Chest. 2025;167(6):1667-1683.