

The expertise in inserting large-bore IV catheters during acute scenarios is essential for doctors, paramedics, and nurses caring for critically ill or injured patients. Large-bore IV lines are frequently needed in the emergency department, trauma victims, or in the OR when major blood loss is anticipated. Most medical professionals become proficient at establishing small-gauge IV lines over time. However, inserting large-bore catheters, especially in patients requiring substantial IV fluids or blood for resuscitation, presents a greater challenge. One might assume that cannulating these prominent, large veins would be straightforward. However, they can be challenging and require skill and expertise.
Characteristics of large veins
- Elasticity: Larger veins may exhibit wall elasticity, which may cause them to “roll” or shift away from the needle during puncture attempts.
- Wall thickness: The walls of larger veins are thicker, requiring more force to penetrate, increasing the risk of rolling or going through the posterior wall of the vein.
- Surrounding tissue: Around larger veins, there might be more surrounding adipose tissue or muscle, making them harder to visualize and access.
- The angle of approach: The optimal angle for cannulating larger veins may differ from that of smaller veins, requiring adjustments in technique.
- Risk of complications: A failed attempt at cannulating a large vein carries a larger risk of complications such as hematoma formation, further complicating subsequent attempts.
- Catheter length: The typically longer length of large-bore catheters makes the insertion technique and handling more challenging.
Successful cannulation, especially in challenging or emergency scenarios, requires knowledge, skill, and the appropriate technique. Here are some general strategies and techniques that can be employed to enhance success rates in cannulating large veins with large-bore IV catheters.
- Traction technique: Applying gentle downward traction on the skin distal to the insertion site can help stabilize rolling veins and make them tenser and easier to puncture. However, be careful here; use firm yet gentle traction to prevent compression of the vein’s volume, making it much more difficult to cannulate.
Large IV catheter (14G), insertion, and technique of stabilizing the skin by digital traction before needle-catheter insertion.
- Bevel-up needle: Starting with the bevel facing up will facilitate the ease of vein entry and decrease the risk of skimming over the vein. Bevel-up also helps the blood enter the needle quicker and appear in the flashback chamber. Rationale: A bevel-down approach may obstruct the bevel with the vein’s intima, causing delayed flushing or unnoticed needle passage through the vein.
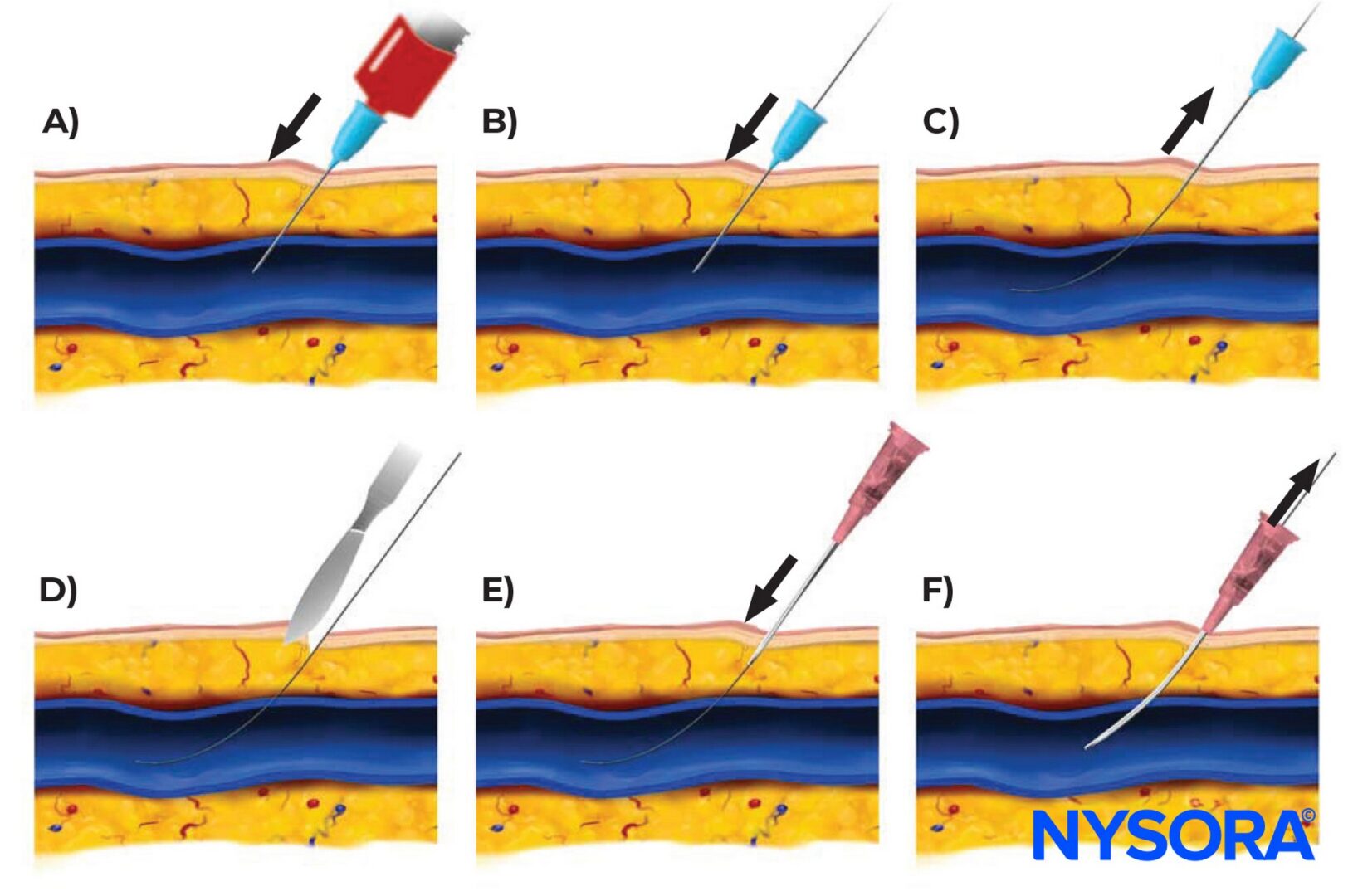
- Seldinger technique: For difficult cannulations, the modified Seldinger technique, involving guidewire insertion followed by the catheter, can be useful.

The Seldinger technique, involving guidewire insertion followed by the catheter, can be useful when cannulating larger veins. A) Needle insertion into the vein. B) Guidewire insertion. C) Needle removal. D) Using a skin dilator or scalpel “nick” (optional). E) The catheter is slid over the guidewire. F) The guidewire is removed.
Large veins. More difficult?
Place large-bore IVs correctly with the NYSORA IV Access App.
- Appropriate angle of entry: Traditional books on IV cannulations often advocate beginning with a steeper angle to penetrate the skin, then flattening the angle as the vein is approached. However, we advise against this approach. Using a steep angle to enter the vein may pose challenges in adjusting the needle without unintentionally removing it or going through its posterior (opposite) wall. This quickly leads to hematoma formation, especially in larger veins. Therefore, we advise starting with a low angle to reduce the risk of going through the posterior wall.
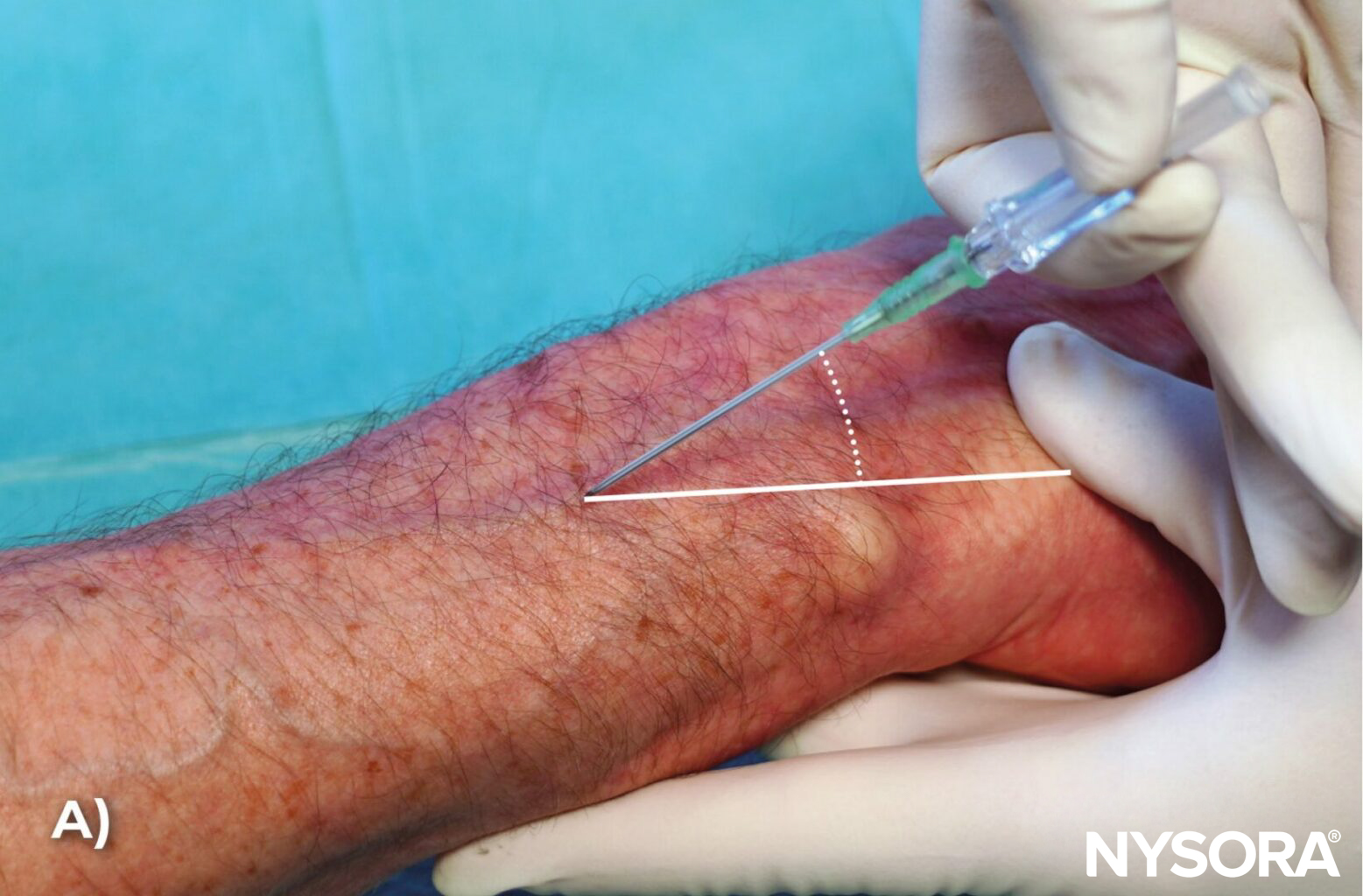

A) Using a steep angle to enter the vein may pose challenges in adjusting the needle without unintentionally removing it or going through its posterior wall. B) Start with a low angle to reduce the risk of going through the posterior wall.
- Stabilize the vein: Using the non-dominant hand to stabilize the vein reduces the likelihood of the vein rolling away. Remember to avoid maneuvers that cause pressure over the vein, which can squeeze the blood out and make it more difficult to cannulate.
- Apply short and controlled fast-forward movements: When encountering resistance while attempting to cannulate the vein, it is imperative to use short, fast, yet controlled forward movements. This approach, we refer to as the “snake bite” technique, helps needle entry through the thick-walled or calcified veins, as opposed to pushing the vein away with a slow approach. Remember that the tips of large bore needle-catheter systems, such as 14G, 16G, or 18G, are not as sharp as the smaller gauge needle tips. As such, they may push the thick-walled veins away from the needle instead of penetrating them. Practicing the snake bite technique is essential for successfully penetrating the vein wall. However, it’s important to ensure these movements are short and controlled to prevent accidental puncture of the vein’s posterior wall.



When inserting a large IV catheter (e.g., 14G), it is imperative to use fast, short, yet controlled forward movements. This will help the needle enter the thick-walled or calcified veins.
- Stay calm and take time: There’s a natural inclination to rush, especially in emergencies. However, staying calm and methodical leads to better outcomes at venous cannulation.
- Ultrasound guidance: Ultrasound guidance allows for real-time visualization of the vein, adjacent structures, and the needle trajectory. Ultrasound can increase the success rate and decrease complications. However, in urgent situations, like trauma cases, immediate large-bore catheter insertion is often paramount, without the luxury of the additional time required for setting up an ultrasound.
By understanding the inherent challenges of inserting large-bore IV catheters in larger veins and employing these strategies, you can increase the success rates and reduce potential complications.











