Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About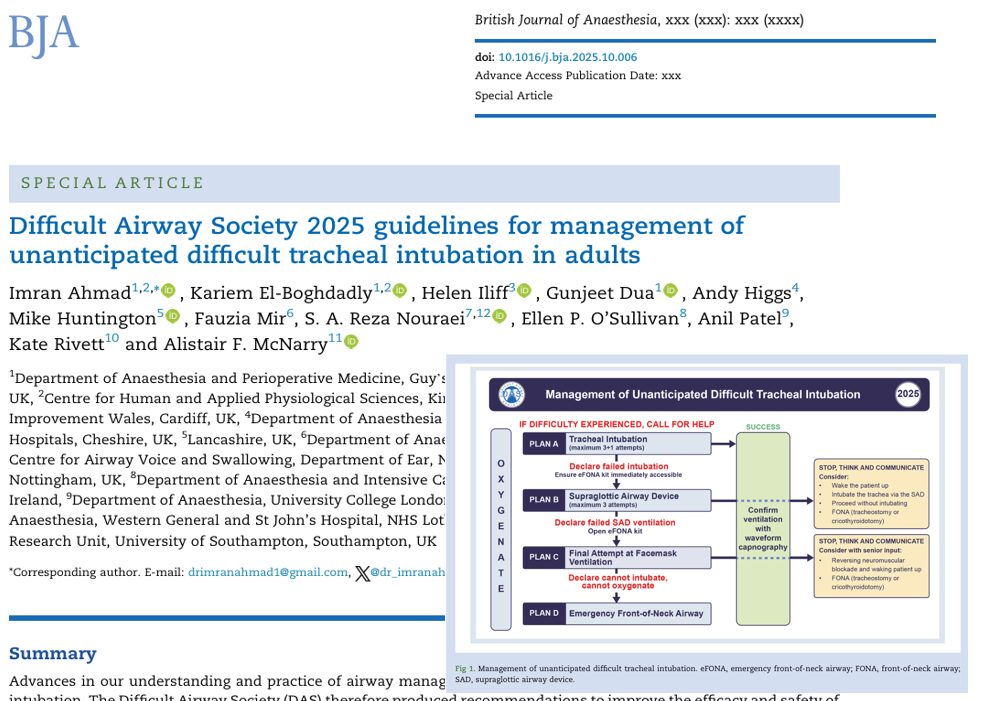





What’s new
The 2025 DAS guideline, titled “Management of unanticipated difficult tracheal intubation in adults”, is a major update authored by Imran Ahmad et al. and published in the British Journal of Anaesthesia.
Key features:
- 1,241 papers reviewed via systematic review, three‑round Delphi process over 3 years.
- 65 recommendations covering major domains: assessment, peroxygenation, human factors, post‑intubation care, and more.
- Maintains the linear algorithm of Plan A → Plan B → Plan C → Plan D (intubation → supraglottic airway → facemask ventilation → emergency front‐of‐neck airway).
- Emphasises maximising success (first pass, oxygenation) rather than only managing failures.
Why this matters
- Unanticipated difficult airway situations remain a key source of perioperative morbidity and mortality; updated evidence means practice must evolve.
- Clinicians now have a modern, evidence‑based tool to guide management when intubation becomes challenging.
- The guideline synthesises technological advances (e.g., videolaryngoscopy, point‑of‑care ultrasound), human factors, and systems thinking into airway management.
Highlighted domains and key changes
1. Pre‑intubation assessment & planning
- The guideline reinforces structured airway assessment AND creates a strategy for the physiologically difficult airway (e.g., shock, severe hypoxia, obesity).
- Planning includes preparation of equipment, team roles, backup plans, and the use of cognitive aids.
2. Peroxygenation and oxygenation strategies
- Continuous oxygen delivery throughout airway management is prioritised.
- Strategies such as high‑flow nasal oxygen, non‑invasive ventilation, and head‑up ramping are given emphasis.
3. First‑pass success and device strategy
- The document emphasises maximising first‑attempt intubation success using appropriate tools and techniques.
- Universal use of videolaryngoscopy is increasingly expected, and the guideline incorporates evidence for this.
4. Using the algorithm: Plan A to D
- Plan A: Tracheal intubation.
- Plan B: Supraglottic airway device ventilation.
- Plan C: Facemask ventilation.
- Plan D: Emergency front‑of‑neck airway (eFONA).
- The guideline reinforces the importance of rapid progression through plans if failure occurs, and clear criteria for when to move to the next plan.
5. Human factors, teamwork & training
- A strong focus on non‑technical aspects: team briefing, role assignment, simulation training, and clear documentation.
- The guideline emphasises that improving success is not only about devices, but about systems and people.
6. Post‑intubation care & documentation
- After successful airway management, the guideline emphasises confirming placement (waveform capnography), monitoring ventilation and oxygenation, and documenting what happened (including a plan if further airway difficulty).
Quick‑reference summary: what should your team do?
-
Pre‑intubation preparation:
- Perform airway assessment & mark potential difficulties.
- Ensure equipment (videolaryngoscope, bougie/stylet, supraglottic devices, eFONA kit), team roles, and plan are ready.
- Preoxygenate thoroughly; consider a ramped position for obesity or physiology‑challenged patients.
- Perform airway assessment & mark potential difficulties.
-
Intubation attempt (Plan A):
- Use videolaryngoscopy as first‑line where available.
- Aim for first‑pass success.
- If unsuccessful within defined attempts/time, transition to Plan B.
- Use videolaryngoscopy as first‑line where available.
-
Plan B / Plan C:
- Insert a supraglottic airway device if intubation fails (Plan B).
- If that fails, consider facemask ventilation (Plan C) — but know when to move forward.
- Insert a supraglottic airway device if intubation fails (Plan B).
-
Plan D – eFONA:
- If you are in a “cannot intubate, cannot oxygenate” scenario, proceed with emergency front‑of‑neck airway without delay.
- Every team member must know this plan and how to execute it.
- If you are in a “cannot intubate, cannot oxygenate” scenario, proceed with emergency front‑of‑neck airway without delay.
-
Post‑intubation & handover:
- Confirm tube placement with capnography.
- Monitor oxygenation, ventilation, and hemodynamics.
- Document the airway course, what device was used, why the failure occurred (if applicable), and plan for extubation/next airway.
- Debrief with the team for learning.
- Confirm tube placement with capnography.
Implementation tips for your department
- Step 1: Disseminate the guideline among your anesthesia and airway teams (consultants, trainees, OT staff, ICU staff).
- Step 2: Review your airway equipment check‑lists: include videolaryngoscope (if available), bougie/stylet, supraglottic devices, eFONA kit, oxygenation adjuncts.
- Step 3: Update your airway algorithms and posters in operating theatres and ICU to reflect Plan A→B→C→D and the emphasis on first‑pass success.
- Step 4: Plan simulation sessions that include unanticipated difficult intubation scenarios, focus on teamwork, human factors, and transitions between plans.
- Step 5: Audit your airway events: track first‑pass success rate, number of attempts, rescue device usage, eFONA usage, complications; feed back to your team.
- Step 6: Ensure documentation templates capture the airway plan, what was used, any difficulties, how they were managed, and the extubation/handover plan.
Final thoughts
The 2025 DAS guideline marks a significant step forward in adult airway management by combining up‑to‑date evidence, a clear algorithmic structure, and a strong emphasis on maximising success rather than just managing failure. For anesthetists, intensivists, and emergency airway practitioners, this is a must‑read.
By embedding these recommendations into your department’s workflow, you can help improve patient safety, team performance, and outcomes in one of the highest‑risk moments in perioperative care.
Reference: Ahmad I et al. Difficult Airway Society 2025 guidelines for management of unanticipated difficult tracheal intubation in adults. Br J Anaesth. Published online November 7, 2025.
Read more about this topic in the Anesthesia Updates section of the Anesthesia Assistant App.