






Malignant hyperthermia (MH) remains one of the most feared complications in anesthesia, rapidly progressive, potentially lethal, and frequently occurring without warning in previously healthy patients. In response to evolving clinical practices and growing understanding, the European Malignant Hyperthermia Group (EMHG) has released an updated guideline on the recognition and management of MH crises.
What is malignant hyperthermia?
Malignant hyperthermia is a rare, life-threatening pharmacogenetic disorder of skeletal muscle metabolism. It is typically triggered by certain anesthetic agents, leading to uncontrolled calcium release within myocytes, which causes hypermetabolism, muscle rigidity, and hyperthermia.
Common triggering agents
- Volatile anesthetic gases (e.g., sevoflurane, desflurane)
- Succinylcholine (a depolarizing muscle relaxant)
These agents can precipitate an MH crisis in genetically susceptible individuals even if they’ve previously undergone uneventful anesthesia.
Recognizing a malignant hyperthermia crisis
Timely recognition is critical. The EMHG stresses the importance of identifying a pattern of signs rather than relying on a single symptom.
Early signs
-
Metabolic:
- Sudden, inappropriate rise in CO₂ production (e.g., elevated end-tidal CO₂)
- Increased oxygen consumption
- Mixed metabolic and respiratory acidosis
- Profuse sweating and skin mottling
- Sudden, inappropriate rise in CO₂ production (e.g., elevated end-tidal CO₂)
-
Cardiovascular:
- Tachycardia (unexplained)
- Ventricular arrhythmias
- Unstable arterial pressure
- Tachycardia (unexplained)
-
Muscular:
- Masseter spasm post-succinylcholine
- Generalized muscle rigidity
- Masseter spasm post-succinylcholine
Late signs
- Rapidly increasing core temperature
- Severe hyperkalemia
- Elevated creatine kinase and myoglobin
- Dark urine (myoglobinuria)
- Cardiac arrest
- Disseminated intravascular coagulation (DIC)
Differential diagnoses to consider
- Inadequate anesthesia or analgesia
- Sepsis
- Anaphylaxis
- Thyroid storm
- Pheochromocytoma
- Neuroleptic malignant syndrome
- Serotonin syndrome
- Recreational drug toxicity (e.g., MDMA)
- Equipment malfunction
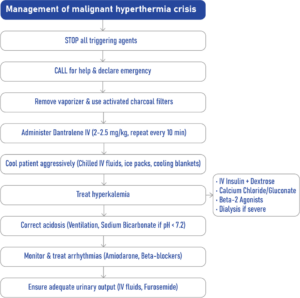
Step-by-step: managing an MH crisis
Immediate intervention (first few minutes)
-
Cease all triggering agents
- Remove volatile agents and discontinue succinylcholine.
-
Ventilate with 100% oxygen
- Use a high flow rate and double to triple the normal minute volume.
-
Call for help and declare an emergency
- Notify the surgical team and consider postponing the procedure.
-
Switch to TIVA (total intravenous anesthesia)
-
Add activated charcoal filters
- Place filters on both inspiratory and expiratory limbs of the anesthesia circuit if available.
Dantrolene: the life-saving antidote
- Initial dose: 2–2.5 mg/kg IV
- Repeat every 10 minutes if symptoms persist, up to a maximum of 300 mg per dose.
- Total dose: May need up to 10 mg/kg or more (maximum ~1200 mg in adults).
- Continue until:
- PaCO₂ < 6 kPa (45 mmHg)
- Decreasing core body temperature
- PaCO₂ < 6 kPa (45 mmHg)
If MH signs recur, continue administering 2–2.5 mg/kg every 10 minutes as needed.
Monitoring and support measures
- Vital monitoring: SaO₂, ECG, blood pressure, ETCO₂, core body temperature
- Lines: Insert arterial line and urinary catheter; consider central venous line
- Labs: Check ABGs, potassium, CK, myoglobin, glucose, renal and hepatic panels, and coagulation studies
- Observe for 24 hours: In critical care or recovery unit due to recurrence risk
Symptomatic treatments
Cooling measures
- Administer 2000–3000 mL of cold crystalloids (4–8°C)
- Use surface cooling devices (e.g., ice packs, cooling blankets)
- Stop cooling when core temp < 38.5°C
Hyperkalemia treatment
- IV insulin + dextrose
- IV calcium chloride or calcium gluconate
- Beta-2 agonists (IV or nebulised)
- Dialysis (in severe cases)
Acidosis treatment
- Hyperventilation to restore normocapnia
- IV sodium bicarbonate if pH < 7.2
Arrhythmia management
- Amiodarone, magnesium
- Beta-blockers (e.g., esmolol) for persistent tachycardia
Urinary output
- Use crystalloids and diuretics like furosemide if necessary to support kidney function and prevent myoglobin-induced nephropathy
New recommendations
Key changes introduced in the 2024 guideline include:
- Flexibility in treatment approaches based on local resources and protocols
- Routine use of activated charcoal filters during suspected MH episodes
- Specific measures for hyperkalemia management
- Updated dantrolene dosing aligned with 2020 EMHG availability recommendations
- Urinary output monitoring and stimulation strategies
Conclusion
The 2024 EMHG guideline on malignant hyperthermia provides a much-needed update tailored to contemporary anesthetic practice. It stresses the need for early recognition, immediate cessation of triggers, prompt administration of dantrolene, and intensive supportive care. With proper training, preparedness, and adherence to these protocols, MH crises can be effectively managed, significantly improving survival rates.
Reference: Glahn KPE et al. Recognition and management of a malignant hyperthermia crisis: updated 2024 guideline from the European Malignant Hyperthermia Group. Br J Anaesth. 2025;134:221-223.
Read more about this topic in the Anesthesia Updates section of the Anesthesia Assistant App.



