


Postoperative pain after video-assisted thoracoscopic surgery (VATS) can be deceptively difficult. Even with an enhanced recovery pathway and multimodal analgesia, many patients report moderate pain during the first hours after surgery—exactly when deep breathing, coughing, and early mobilization are most needed to prevent atelectasis and pneumonia. Regional anesthesia helps close this gap by targeting thoracic wall innervation while avoiding neuraxial risks. Two techniques dominate the current conversation: the surgeon-delivered intercostal nerve block (ICNB), a long-standing method that anesthetizes the anterior rami in specific dermatomes; and the ultrasound-guided erector spinae plane block (ESPB), a popular, superficial fascial plane injection with reputed multilevel spread and a wide safety margin.
Guidelines for VATS increasingly mention ESPB as a component of a balanced regimen, yet its mechanism and clinical signal remain debated: does local anesthetic consistently reach the paravertebral space and ventral rami—or does systemic uptake explain part of the effect? Meanwhile, ICNB is sometimes downplayed due to concerns about rapid systemic absorption and limited duration, despite strong face validity for coverage of the incision/intercostal pain generators. Clinicians are left wondering which approach best reduces opioid needs and pain in the crucial early window after uniportal VATS—without trading off safety.
This multicenter, double-blind, placebo-controlled RCT directly compared surgeon-performed ICNB with ultrasound-guided ESPB for uniportal VATS, testing whether ICNB reduces early morphine use and improves analgesic outcomes.
Study objective and methods
The primary aim of the study was to compare ICNB versus ESPB (each tested against placebo) for analgesia after uniportal VATS; primary endpoint: cumulative morphine use in the first 12 h post-extubation.
- Design: Multicenter, prospective, randomized, double-blind, placebo-controlled superiority trial.
- Setting: Two Belgian centers (University Hospital Leuven; Jessa Hospital, Hasselt) within standardized ERATS pathways.
- Population: 100 adults (ASA I–IV) undergoing elective uniportal VATS (wedge excision or lobectomy). Final analysis n = 98 for primary due to two PCA device errors (retained for safety).
- Groups and masking: At the end of surgery, patients received active ICNB + placebo ESPB or active ESPB + placebo ICNB; patient, block team, and ward staff were blinded; allocation concealed.
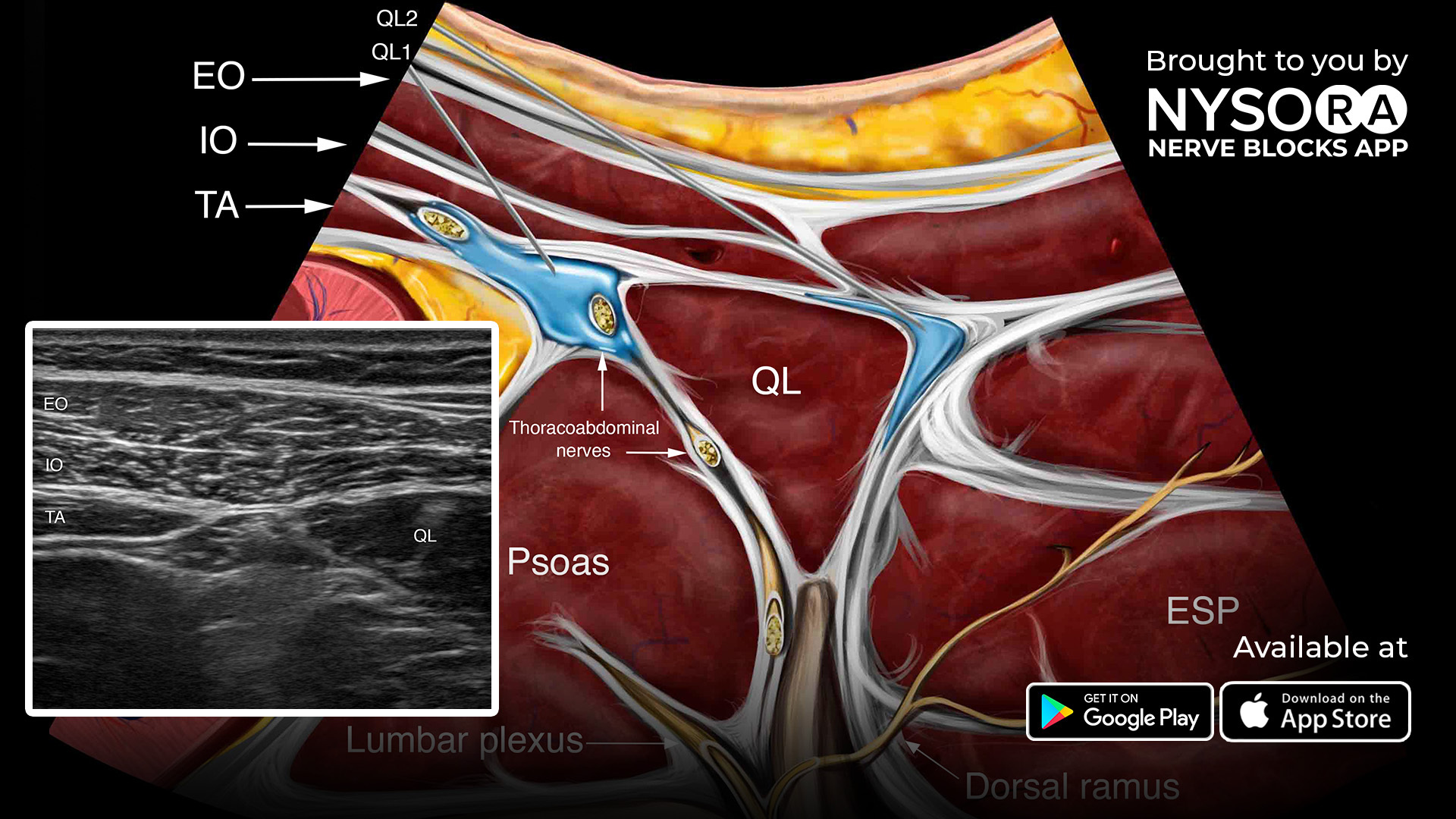
- ICNB (surgical, thoracoscopic): 6–7 levels T5–T11, 30 mL ropivacaine 0.5% total (or saline), typically 3–4 mL/space.
- ESPB (ultrasound-guided): Single-shot at T5–T6, 30 mL ropivacaine 0.5% (or saline) with craniocaudal spread confirmation.
- Perioperative care: Standard ERATS multimodal regimen; all received PCA morphine (on-demand only) for 24 h.
- Primary outcome: Cumulative 12-h morphine consumption (post-extubation).
- Key secondary outcome: 24-h morphine.
- Other secondary outcomes: PACU pain (hourly to 4 h), PCA requests, rescue medication, satisfaction, complications, fit-for-discharge/LOS, and total plasma ropivacaine at 15, 30, and 60 min in a randomized subset. Intention-to-treat analyses with center-stratified tests.
Key findings
-
Primary analgesic endpoint—12 h opioids
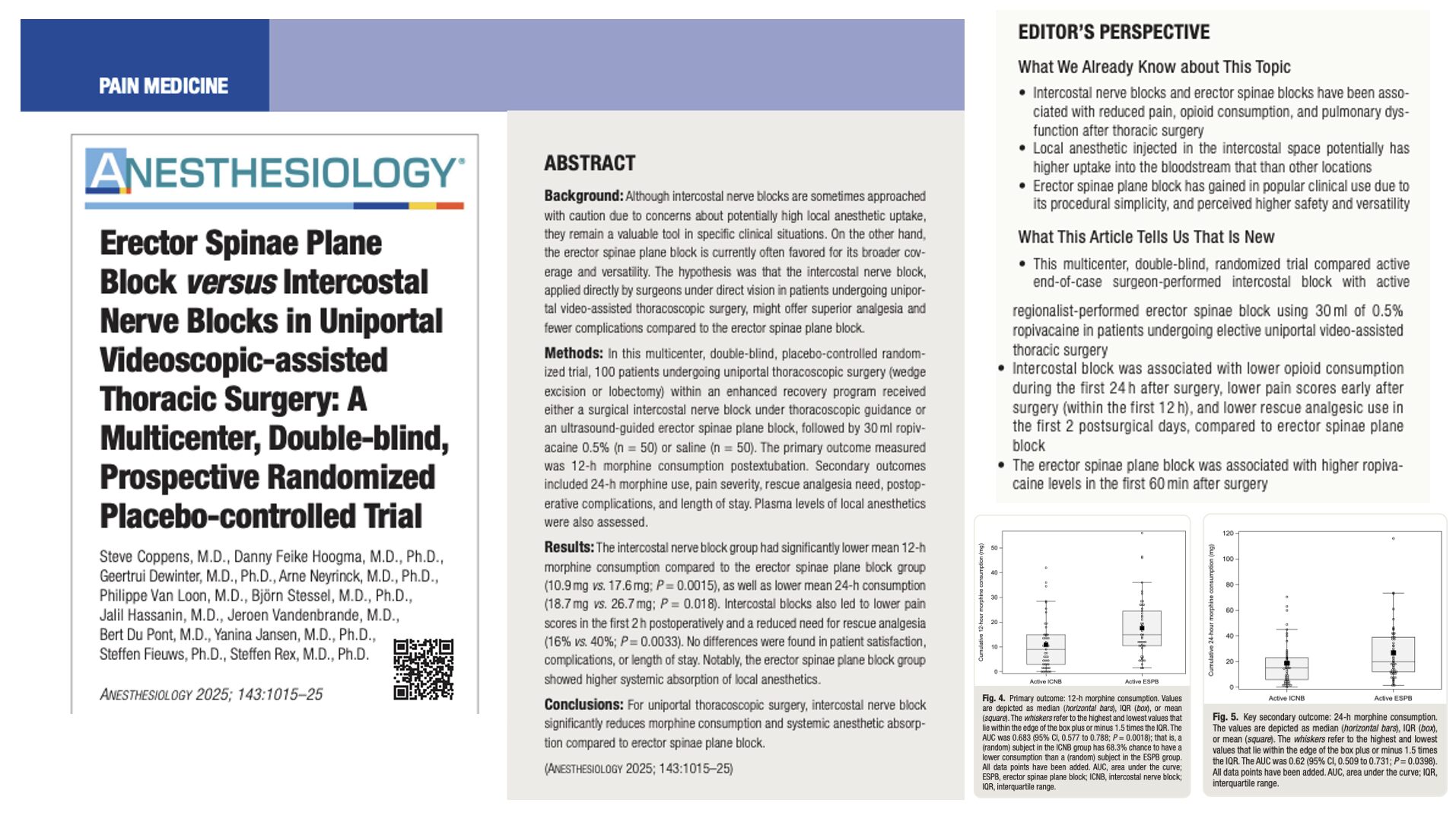
ICNB cut early opioid needs: mean 12-h morphine 10.9 mg (ICNB) vs 17.6 mg (ESPB); difference 6.7 mg (95% CI 2.3–11.2), P = 0.0015. Sensitivity analyses agreed (including log-normal modeling).
-
24 h opioids—benefit persists but attenuates
At 24 h, morphine remained lower with ICNB: 18.7 mg vs 26.7 mg; difference 7.9 mg (95% CI 0.5–15.4), P = 0.018.
-
Early pain scores and rescue needs—ICNB superior in PACU
During the first 2 h in PACU, NRS pain scores were consistently lower with ICNB (significant at 30, 60, 90, and 120 min). Rescue analgesia was required less often with ICNB (16% vs 40%; P = 0.0033) and remained lower on postoperative day 1 (52% vs 76%; P = 0.0178). By 12 and 24 h, median pain scores converged between groups.
-
Systemic local anesthetic exposure—higher with ESPB
Total plasma ropivacaine concentrations were significantly higher after ESPB at 15 and 60 min (and numerically higher at 30 min), with three ESPB patients reaching the 2.2 µg/mL threshold associated with potential neurotoxicity in prior literature (no LAST events observed). The ICNB group had lower systemic levels across time points.
-
Patient-centred and safety outcomes—no separation
Patient satisfaction, complications (including PONV), and fit-for-discharge/hospital LOS were similar. No block-related serious adverse events occurred in either group.
-
Mechanistic implication—coverage where it counts
The authors argue ICNB reliably anesthetizes anterior rami at the port/intercostal levels typical for uniportal VATS, whereas ESPB may act predominantly on posterior rami with variable anterior spread—helping explain better early incisional pain control with ICNB despite ESPB’s popularity.
Conclusion
Within a standardized ERATS pathway for uniportal VATS, surgeon-performed ICNB produced meaningfully lower morphine use at 12 and 24 h, better early PACU pain scores, and fewer rescue requirements than ultrasound-guided ESPB—without increased complications or LOS. Importantly, systemic ropivacaine exposure was higher with ESPB, challenging the assumption that ESPB is always “lighter” systemically than perineural techniques. For the uniportal VATS setting, this trial supports ICNB as the more efficient single-shot choice when the clinical goal is to blunt early movement-related thoracic wall pain and reduce immediate opioid burden.
Future research
- Patient-centred endpoints: Incorporate core outcomes (quality of recovery, sleep, cough peak flow, pulmonary complication composites) to test whether early analgesic gains translate to functional benefits.
- Technique scope: Evaluate findings in multiportal VATS and open thoracotomy; compare single-shot ICNB with continuous catheter strategies or surgeon-delivered multilevel local infiltration.
- Pharmacokinetics: Measure free (unbound) local anesthetic fractions to clarify toxicity risk; dose-finding to balance efficacy with exposure for both ICNB and ESPB.
- Mechanistic imaging: High-resolution imaging or cadaveric correlation to confirm anterior rami coverage and explain inter-individual variability in ESPB spread.
Clinical implications
For uniportal VATS in an ERATS program, ICNB is a pragmatic first-line regional choice when expertise and workflow allow the surgeon to inject under direct thoracoscopic vision at T5–T11. Expect lower early opioid needs (~ 7 mg less by 12 h), better PACU pain control, fewer rescues, and no apparent safety penalty—all while reducing systemic LA exposure relative to ESPB. ESPB remains a useful, versatile block with convenient external access, but its anterior rami/port-level coverage appears less reliable in this context, and systemic uptake can be higher than many assume. Build your pathway around ICNB for uniportal cases, reserving ESPB for scenarios where surgical ICNB is not feasible (e.g., workflow constraints, skill mix) or as an adjunct when broader posterior chest wall analgesia is desired.
Clinical pearls
- ICNB wins early: Lower 12-h and 24-h morphine, better PACU pain scores, fewer rescues.
- Safety comparable: No increase in complications or LOS; satisfaction similar between groups.
- Systemic LA exposure: ESPB yielded higher plasma ropivacaine levels in the first hour.
- Mechanism matters: ICNB targets anterior rami at port levels—high-yield for uniportal VATS pain.
Practical tip: For uniportal VATS, make the surgeon-delivered multilevel ICNB (T5–T11, ~ 3–4 mL per space, 0.5% ropivacaine) your default; use ESPB when ICNB isn’t feasible.
For more detailed information, refer to the full article in Anesthesiology.
Coppens S. et al. Erector Spinae Plane Block versus Intercostal Nerve Blocks in Uniportal Videoscopic-assisted Thoracic Surgery: A Multicenter, Double-blind, Prospective Randomized Placebo-controlled Trial. Anesthesiology. 2025;143:1015-1025.
Download the Nerve Blocks App HERE for in-depth insights on the ICNB and ESPB techniques. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Module on NYSORA360!