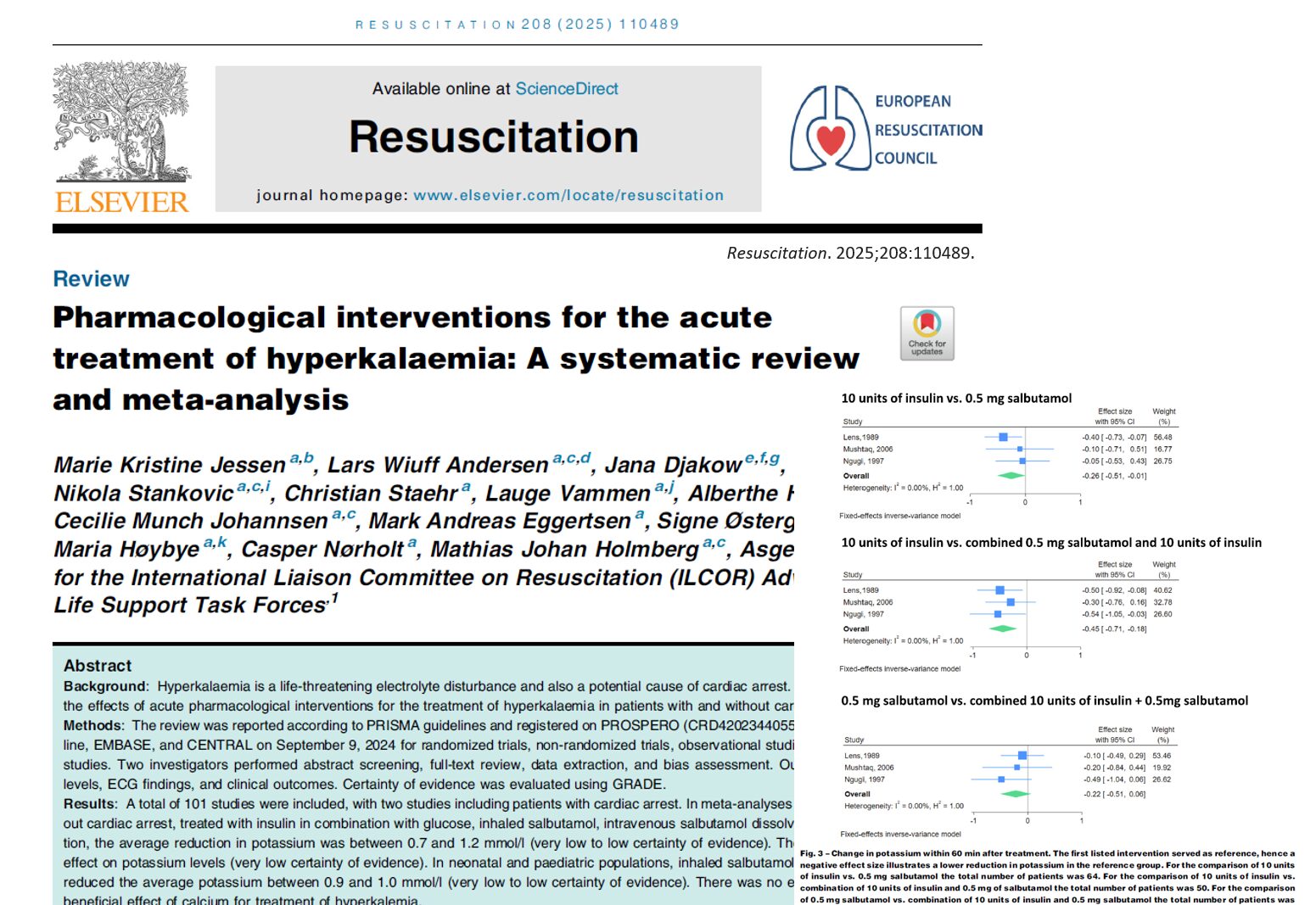

Hyperkalemia, a potentially fatal electrolyte disorder characterized by elevated serum potassium levels, remains a significant challenge in clinical practice. A newly published systematic review and meta-analysis (Jessen et al., 2025) has now meticulously examined the efficacy of various pharmacological interventions in treating acute hyperkalemia, including cases with and without cardiac arrest. The results provide crucial insights into optimal treatment strategies, raising questions about some long-standing clinical practices.
What is Hyperkalemia?
- Definition:
- Adults: Serum potassium ≥ 6.5 mmol/L (Severe Hyperkalemia)
- Neonates/Premature neonates: Serum potassium ≥ 6.0–6.5 mmol/L
- Normal range: 3.5 – 5.0 mmol/L
- Risks: Severe hyperkalemia may cause life-threatening arrhythmias and sudden cardiac death.
Effective pharmacological interventions
1. Insulin with Glucose/Dextrose
- Mechanism: Facilitates transcellular shift of potassium into cells.
- Adult population:
- 10 units insulin + glucose reduced potassium by 0.7 – 1.4 mmol/L within 60 minutes.
- Meta-analysis result: Average potassium reduction of 0.7 mmol/L.
- Neonatal/Pediatric population: Weight-based approaches showed variable results.
2. Beta2-Agonists (Salbutamol/Albuterol)
- Inhaled Salbutamol:
- Adults:
- Doses: 10–20 mg inhaled
- Potassium reduction: −0.9 mmol/L
- Neonates/Pediatrics:
- 400 mcg of inhaled salbutamol reduced potassium by −0.9 mmol/L.
- Intravenous Salbutamol:
- Adults:
- 0.5 mg IV salbutamol (dissolved in glucose): −1.0 mmol/L potassium reduction.
- Combining IV salbutamol with insulin + glucose resulted in −1.2 mmol/L reduction.
- Neonates/Pediatrics:
- 4–5 mcg/kg IV salbutamol reduced potassium by −1.0 mmol/L.
3. Combination therapies
- Insulin + IV Salbutamol (0.5 mg) + Glucose:
- Superior to insulin alone.
- Potassium reduction: Up to −1.2 mmol/L within 60 minutes.
Ineffective or uncertain interventions
1. Bicarbonate
- Five adult studies showed no significant potassium reduction (mean change: −0.1 mmol/L).
2. Calcium (Calcium Chloride/Gluconate)
- No evidence supporting clinical benefit in hyperkalemia management.
- Some observational studies suggest possible worse outcomes during cardiac arrest, but results have a high risk of bias.
- Traditionally used to stabilize myocardial cells but lacks concrete evidence for improving survival outcomes.
Acute management of Hyperkalemia (Non-Cardiac Arrest)

Conclusion
While insulin combined with glucose and beta2-agonists remains the cornerstone of acute hyperkalemia management, routine use of calcium or bicarbonate may need re-evaluation. Future high-quality randomized trials focusing on patient-centered outcomes, especially in cardiac arrest and pediatric settings, are urgently required to further refine treatment guidelines.
Reference: Jessen MK, Andersen LW, Djakow J, et al. Pharmacological interventions for the acute treatment of hyperkalaemia: A systematic review and meta-analysis. Resuscitation. 2025;208:110489
For more information on hyperkalemia management, check out Anesthesia Updates on the NYSORA Anesthesia Assistant App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.
We asked Anesthesia Assistant App’s Case Manager:
We have a 68-year-old patient with chronic kidney disease. The patient shows a potassium of 6.8 mmol/L, wide QRS on ECG, borderline hypotension.