A 2025 study published in the European Journal of Anaesthesiology has introduced a rigorously developed 19-point safety checklist for using high-flow nasal oxygen (HFNO) in apnoeic oxygenation during laryngotracheal surgery. Developed through an international Delphi consensus process, this tool aims to standardize practice, improve patient safety, and support multidisciplinary teams in delivering optimal care during complex airway procedures.
Why this matters
Apnoeic oxygenation using HFNO, once known by its trademark acronym THRIVE (Transnasal Humidified Rapid-Insufflation Ventilatory Exchange), has revolutionized the way laryngeal and tracheal surgeries are performed:
- It enables tubeless airway surgery by avoiding the need for endotracheal intubation.
- It prolongs apnoea time, offering surgeons better visual and operative access.
- It delivers warmed, humidified oxygen at high flow rates, reducing mucosal drying and improving patient comfort.
However, despite widespread clinical adoption, there has been no unified protocol or safety guideline until now.
What’s in the checklist?
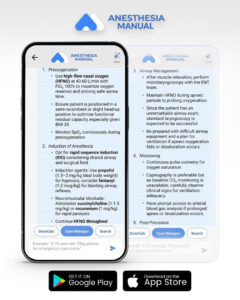
The final checklist includes 19 essential items, grouped across three phases of care:
Pre-procedure (11 items)
- Assess patient suitability early (surgical pathology, obesity, airway anatomy)
- Multidisciplinary team briefing to:
- Confirm suitability
- Agree on a rescue oxygenation plan
- Define SpO₂ threshold for intervention
- Use the WHO Surgical Safety Checklist alongside the HFNO checklist
- Preoxygenation using HFNO:
- FiO₂ = 1.0
- Flow ≥ 50 L/min (ideally 70 L/min)
- Minimum 5 minutes
- Encourage closed-mouth breathing
- Confirm SpO₂ reaches 100% (or agreed target)
- Ensure carbon dioxide monitoring is available
- Set up operating room ergonomics and all rescue airway devices:
- Facemask
- Supraglottic airway
- Laryngoscope
- Jet ventilation (if applicable)
Peri-procedure (4 items)
- Use total intravenous anesthesia (TIVA); recommend rocuronium
- Maintain upper airway patency with jaw thrust or oropharyngeal airway
- Confirm facemask ventilation effectiveness pre-surgery
- Begin surgery while ensuring continued airway patency
Post-procedure (4 items)
- Be prepared to regain airway control post-op with adjuncts or intubation
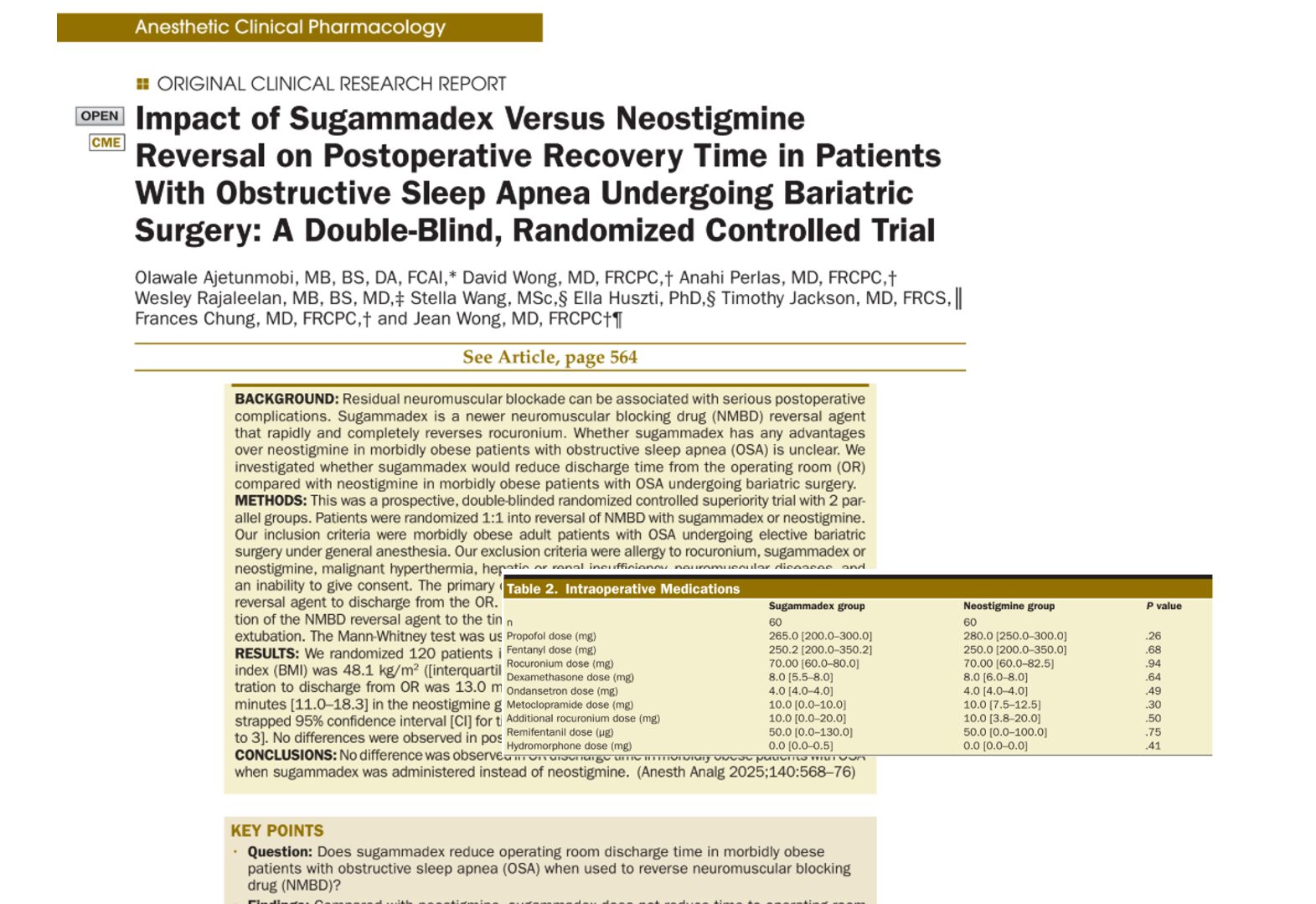
- Reverse neuromuscular block (use sugammadex for rocuronium)
- Ensure spontaneous ventilation is re-established before PACU transfer
- Consider continuing HFNO during recovery for patients at risk of edema or obstruction
Why standardization is critical
Although HFNO is increasingly used for apnoeic oxygenation, studies have identified risks, including:
- Carbon dioxide accumulation: CO₂ clearance is minimal during true apnoea, increasing the risk of acidosis.
- Unexpected desaturation: Particularly in obese or anatomically complex patients.
- Inadequate preparation: Variability in clinician experience and lack of rescue strategies.
The checklist helps mitigate these by encouraging proactive planning, monitoring, and teamwork.
Key practice pearls
What’s the ideal patient profile?
- Normal or moderately elevated BMI
- No significant pulmonary shunt physiology
- Stable cardiovascular status
- Anticipated short-to-moderate surgical duration
High-risk features:
- Obesity (BMI > 35)
- Baseline hypoxemia (SpO₂ < 95%)
- Restrictive lung disease
- Anticipated difficult airway or rescue plan
- Long surgical duration
Equipment readiness:
- Confirm the flow and heat function on the HFNO device
- Have suction, mask ventilation, and intubation tools ready
- Consider the use of flow-diversion nasal cannulae (e.g., Optiflow Switch™) to allow bag-mask ventilation without removing nasal prongs
Training and teamwork
The checklist emphasizes the importance of:
- Multidisciplinary coordination
- Clear role assignments
- Simulation training to enhance familiarity with HFNO workflows and rescue protocols
Incorporating the checklist into team briefs and surgical time-outs promotes situational awareness and reduces last-minute confusion.
Final thoughts
The introduction of this consensus-driven safety checklist marks a significant advancement in airway surgery safety. It distills expert knowledge into a practical format, enabling teams to deliver HFNO-based apnoeic oxygenation more reliably and safely.
In an era of precision and protocolized medicine, this tool fills a long-standing gap, bringing structure, safety, and clarity to a technique used in high-stakes surgical scenarios.
Reference: Ghosh P. et al. HFNO expert consensus group. A safety checklist for apnoeic oxygenation using high-flow nasal oxygen for laryngotracheal surgery in adults: An international Delphi consensus. Eur J Anaesthesiol. 2025;42:357-365.
For more information on HFNO and new guidelines, check out Anesthesia Updates on the NYSORA Anesthesia Manual App.
Get access to step-by-step management algorithms, the latest research, and peer-reviewed insights—all in one place. Download the app today and experience the future of anesthesia education and decision-making.
AI on call: Case of the week
A 58-year-old man is scheduled for elective microlaryngoscopy with biopsy of a vocal cord lesion. He is a smoker with well-controlled hypertension and a BMI of 33. Preoperative airway exam is unremarkable. The ENT team requests apnoeic oxygenation using high-flow nasal oxygen (HFNO) to optimize surgical exposure. The patient has a SpO₂ of 94% on room air, and no baseline CO₂ monitoring is available in the OR.