Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App VetRA App
VetRA App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About
Learning objectives
- Describe the pathophysiology and symptoms of hyperthyroidism
- Diagnose and treat hyperthyroidism
- Manage patients with hyperthyroidism or thyroid storm
Background
- Hyperthyroidism is a syndrome associated with excess thyroid hormone production
- Can lead to thyroid storm, an acute and life-threatening complication
- Most commonly caused by Graves disease (young population) and toxic multinodular goiter (older population)
- Other causes: Iodine-induced hyperthyroidism (Jod-Basedow phenomenon), thyroid adenomas, de Quervain thyroiditis (subacute thyroiditis), postpartum thyroiditis, factitious thyroiditis (thyrotoxicosis factitia)
Pathophysiology
- Graves disease
- Thyroid-stimulating antibodies mimicking the effects of thyroid-stimulating hormone (TSH)
- Typical signs: Edema of retro-orbital tissues, pretibial myxedema
- Toxic multinodaular goiter
- Palpable thyroid nodules leading to excess thyroid hormone production
- Thyroid adenoma
- Solitary palpable module causing hyperthyroidism
- Thyroiditis
- Transient increase in circulating thyroid hormone resulting from mechanical disruption of thyroid follicles
- Iodine-induced hyperthyroidism
- Typically iatrogenic
- Due to administration of iodine-containing medications (e.g., contrast media, amiodarone)
Signs & symptoms
- Weight loss despite increased appetite
- Palpitation
- Nervousness
- Tremors
- Dyspnea
- Fatigability
- Diarrhea
- Increased gastrointestinal motility
- Muscle weakness
- Heat intolerance
- Diaphoresis
- Goiter
- Palpable nodules
- Painful thyroid
Diagnosis
- Initial test: Serum TSH (decreased)
- Free T3 and T4 (increased)
- ECG when atrial fibrillation is suspected
- Palpitation of the thyroid gland
- 24-hour radioactive iodine (RAIU) uptake to distinguish between etiologies
- Increased RAIU: Graves disease, toxic multinodular goiter, thyroid adenoma
- Decreased RAIU: Subacute thyroiditis, painless thyroiditis, iodine-induced hyperthyroidism, factitious hyperthyroidism
- Thyroid receptor antibody measurement as an alternative diagnosis for Graves disease
- Radioisotope thyroid scan
Treatment
- Symptomatic
- Beta-blockers or calcium channel blockers
- Definitive
- Radioactive iodine
- Thionamide
- Subtotal thyroidectomy
- Clinical assessment and free T4 monitoring are essential for all treatments
Anesthetic management
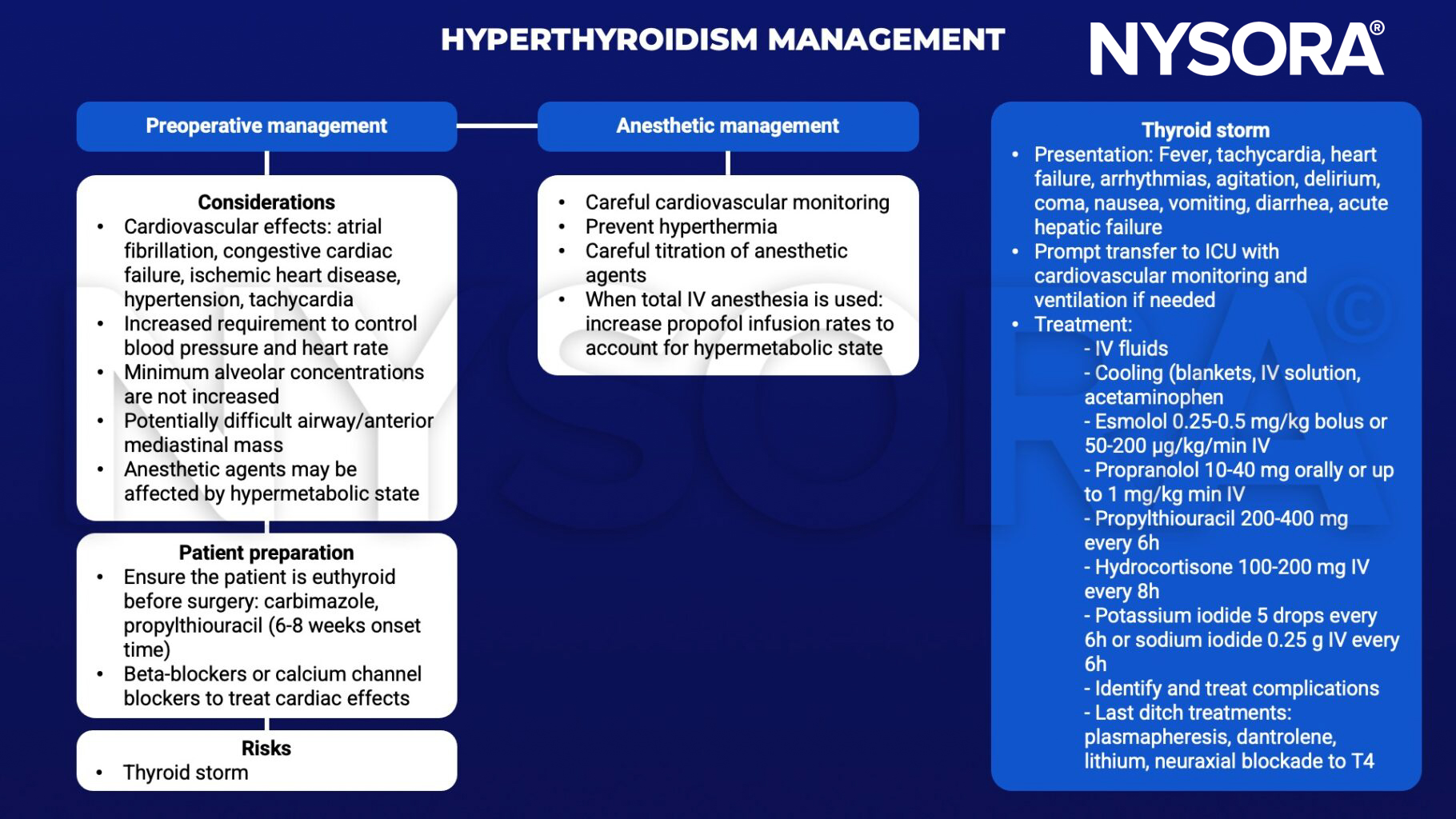
Keep in mind
- Acute coronary syndrome may be complicated with thyroid dysfunction
- Close monitoring is essential with propylthiouracil administration in pregnant patients as overcorrection can potentially cause fetal hypothyroidism
Suggested reading
- Pokhrel B, Aiman W, Bhusal K. Thyroid Storm. [Updated 2022 Oct 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448095/
- Mathew P, Rawla P. Hyperthyroidism. [Updated 2022 Jul 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537053/
- Carroll R, Matfin G. Endocrine and metabolic emergencies: thyroid storm. Ther Adv Endocrinol Metab. 2010;1(3):139-145.
- Farling PA. Thyroid disease. BJA: British Journal of Anaesthesia. 2000;85(1):15-28.
Clinical updates
Shao et al. (BMC Anesthesiology, 2024) report that thyroid storm can occur during or after non-thyroid surgery in patients with previously unrecognized or subclinical hyperthyroidism, often presenting intraoperatively under general anesthesia as refractory tachycardia with minimal or atypical systemic signs. Their case review highlights that more than half of perioperative thyroid storm cases followed missed preoperative diagnosis, emphasizing the need for meticulous history taking, early consideration of thyroid dysfunction when unexplained tachycardia or hyperthermia occurs, and prompt initiation of β-blockade, antithyroid drugs, steroids, and supportive care once thyroid storm is suspected.