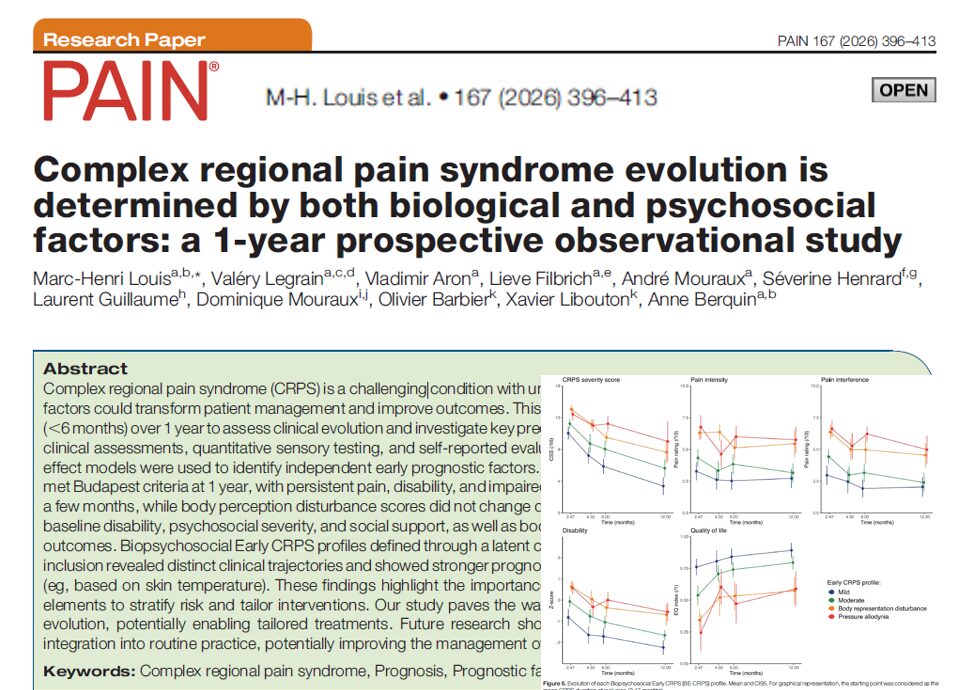

A major prospective study of patients with early complex regional pain syndrome (CRPS) (Louis et al., Pain 2026) has revealed that certain physical, psychological, and demographic factors present at diagnosis can strongly influence how the disease evolves over time. The results challenge long-held assumptions and provide a new framework for early intervention strategies in CRPS.
The findings, based on 251 patients across eight European centers and followed for a full year, show that pain intensity alone is not the primary predictor of long-term CRPS outcomes. Instead, initial disability, high body mass index (BMI), and mental health factors like anxiety emerged as stronger predictors of chronic disease persistence and functional impairment.
What is CRPS?
Complex regional pain syndrome (CRPS) is a rare but debilitating condition, often triggered by trauma or surgery. It is characterized by intense, chronic pain, swelling, changes in skin color and temperature, and motor dysfunction, typically affecting one limb. CRPS is classified into:
- CRPS type I: No confirmed nerve injury
- CRPS type II: Confirmed nerve injury
CRPS affects quality of life dramatically and has long been considered a disease of disproportionate, poorly understood pain responses.
Study background and objectives
This prospective, observational study was conducted by the EU-funded BioPain project to evaluate longitudinal outcomes in CRPS and identify early predictive factors.
Study design:
- Participants: 251 adults with early CRPS (≤1 year since onset)
- Duration: 1-year follow-up
- Sites: 8 academic pain centers in Europe
- Main outcomes: Pain intensity, motor dysfunction, disability (Brief Pain Inventory), and CRPS severity
The authors aimed to:
- Measure natural disease progression over 12 months
- Identify predictors of poor or persistent outcomes
Key findings at a glance
- Disability, not pain, predicted poor long-term outcomes
- High BMI, older age, and anxiety were strong predictors of persistent CRPS
- Women were overrepresented (77% of the cohort), aligning with prior CRPS demographics
- Most improvement occurred in the first 3 months, with stability or plateau after that
1. Pain is not the best predictor of CRPS evolution
Contrary to conventional focus on pain intensity, the study found no direct correlation between baseline pain levels and poor outcomes at 12 months.
Instead, the most consistent predictors of chronic impairment were:
- Initial functional disability
- Poor limb movement
- High BMI
- Psychological distress, especially anxiety
2. Disability, motor impairment, and BMI drive chronicity
At baseline, many participants already had significant functional impairments. The Brief Pain Inventory – Interference scale (BPI-I) was a strong marker for predicting poor outcomes.
Top predictors of poor CRPS outcome:
- High BPI-Interference scores
- Abnormal limb movement (e.g., dystonia, bradykinesia)
- High BMI (>30)
- Older age (especially >50 years)
These findings suggest that systemic health and physical function are more influential on recovery than pain severity alone.
3. Psychological distress plays a key role
Mental health symptoms were common in the cohort:
- Anxiety was more predictive than depression of poor recovery.
- Pain catastrophizing was also significantly associated with worse disability.
- Stress and sleep disturbances compounded outcomes.
According to the study, patients with moderate to high anxiety had nearly double the risk of long-term disability.
This reinforces the importance of a biopsychosocial model in treating CRPS, where addressing psychological distress is as essential as managing pain.
4. Female gender and limb affected show trends
While not statistically significant in all models, the study observed the following trends:
- Female patients had slightly higher rates of persistent disability.
- Upper-limb CRPS was associated with slower motor recovery than lower-limb CRPS.
These findings align with previous research suggesting hormonal, behavioral, or diagnostic factors may influence female vulnerability and regional differences in disease course.
Early interventions to consider
Based on the study’s results, here are 5 evidence-informed strategies clinicians should consider within the first 3 months of CRPS diagnosis:
- Evaluate and monitor disability using tools like the BPI-I to detect high-risk patients.
- Screen for anxiety and stress, using validated tools like HADS or PCS.
- Encourage movement early, even if painful, to prevent dystonia and motor deterioration.
- Address BMI and overall metabolic health, as obesity was a key predictor of poor recovery.
- Provide interdisciplinary care, including physical therapy, psychology, and pain management.
Clinical implications
The study reframes CRPS from a purely pain-focused condition to one requiring a multifactorial assessment from day one.
Take-home messages:
- Pain severity is not the sole or best predictor of CRPS evolution.
- Disability, movement disorders, BMI, and anxiety should be prioritized in early assessment.
- A short window exists (0–3 months) for aggressive early intervention.
- Functional recovery, not just pain relief, should be the primary treatment goal.
Limitations of the study
While robust in design, the study acknowledges a few limitations:
- No treatment standardization: Patients received varying therapies, making it harder to assess intervention effectiveness.
- Limited to European academic centers, which may not represent general community practice.
- Dropout rate of ~20%, although statistical methods accounted for this.
Still, the multicenter nature and prospective design provide one of the most comprehensive real-world snapshots of early CRPS outcomes to date.
Future directions
The authors call for:
- Randomized trials targeting identified risk factors, such as anxiety and obesity
- Longer follow-up (>2 years) to assess chronicity beyond the 12-month mark
- Biomarker studies to explore the neuroinflammatory or metabolic contributors to CRPS chronicity
- Early intervention programs combining physical and psychological rehabilitation.
Conclusion
This pivotal 1-year study shifts the lens on CRPS from a pain-centered model to a function-centered, biopsychosocial approach. By identifying early red flags such as poor movement, obesity, and anxiety, clinicians can better triage patients at risk for persistent disability.
It underscores the urgent need to screen broadly, intervene early, and treat holistically, offering hope for patients with what has long been considered an enigmatic and untreatable condition.
For more information, refer to the full article in PAIN.
Louis MH, Legrain V, Aron V, et al. Complex regional pain syndrome evolution is determined by both biological and psychosocial factors: a 1-year prospective observational study. Pain. 2026;167(2):396-413.
For detailed guides on interventions used in the treatment of CRPS, download NYSORA’s Ultrasound Pain App!