Knee osteoarthritis (OA) is a degenerative joint disease that significantly impairs mobility and quality of life in millions of individuals worldwide. Traditional management strategies, such as physical therapy, non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroid injections, and eventually, total knee arthroplasty, often fall short in providing lasting relief, especially for patients ineligible for surgery.
Recent innovations like radiofrequency ablation (RFA) and intra-articular mesenchymal stem cell (MSC) injections offer hope. A 2025 network meta-analysis by Park et al., published in Regional Anesthesia & Pain Medicine, provides a comprehensive comparison of these two advanced therapies.
Understanding knee osteoarthritis and its treatment gaps
OA is a degenerative joint disorder characterized by:
- Progressive loss of articular cartilage
- Subchondral bone remodeling
- Synovial inflammation
- Osteophyte formation
Symptoms include:
- Chronic knee pain
- Joint stiffness
- Swelling and reduced range of motion
- Functional limitations
Conventional treatments include:
- Physical therapy
- Oral NSAIDs (e.g., ibuprofen, celecoxib)
- Intra-articular corticosteroids (IACS)
- Hyaluronic acid injections (IAHA)
- Platelet-rich plasma (PRP)
These modalities have shown only moderate or short-lived benefits, prompting exploration into alternatives like RFA and MSC therapy.
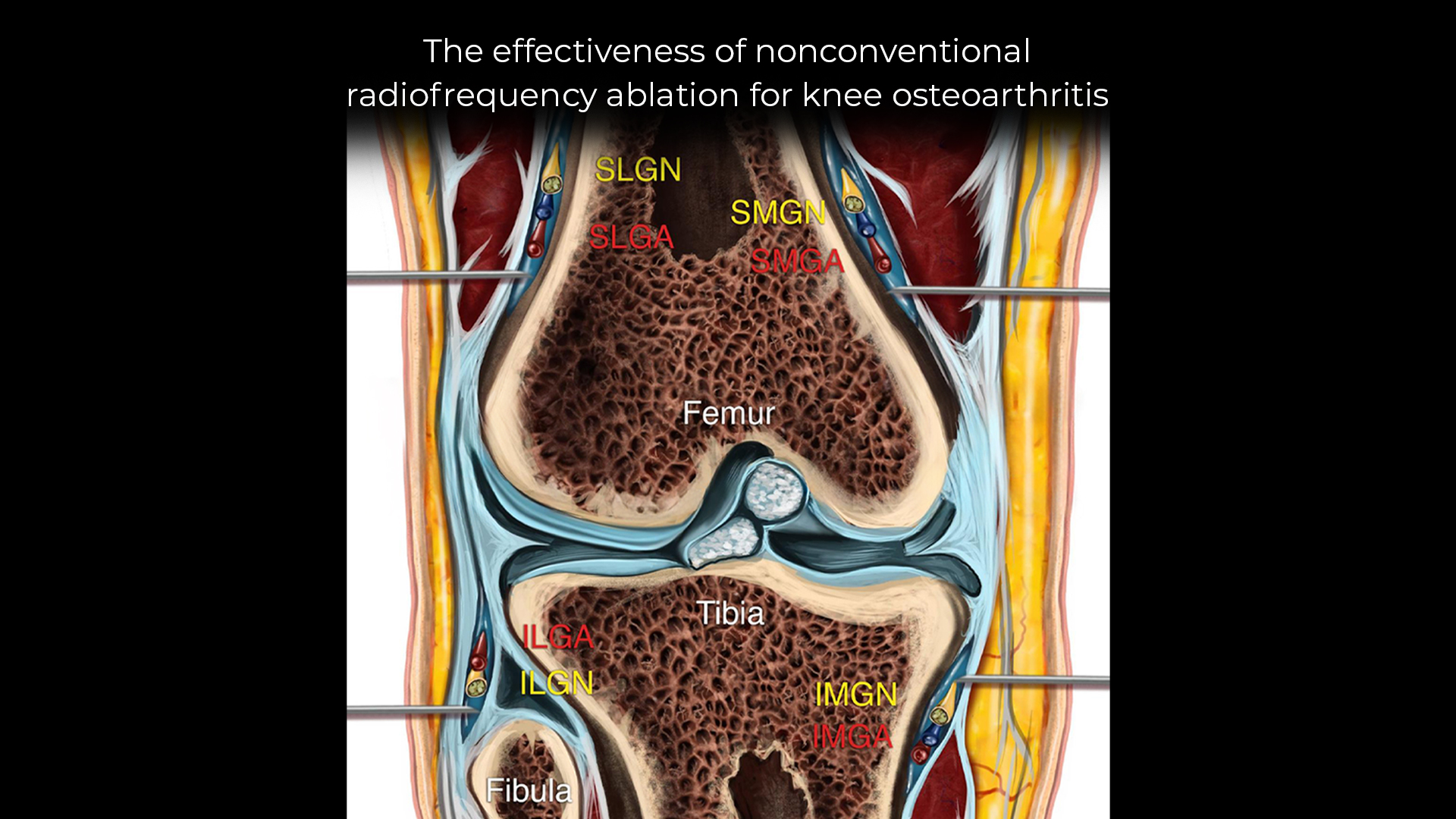
Radiofrequency ablation (RFA)
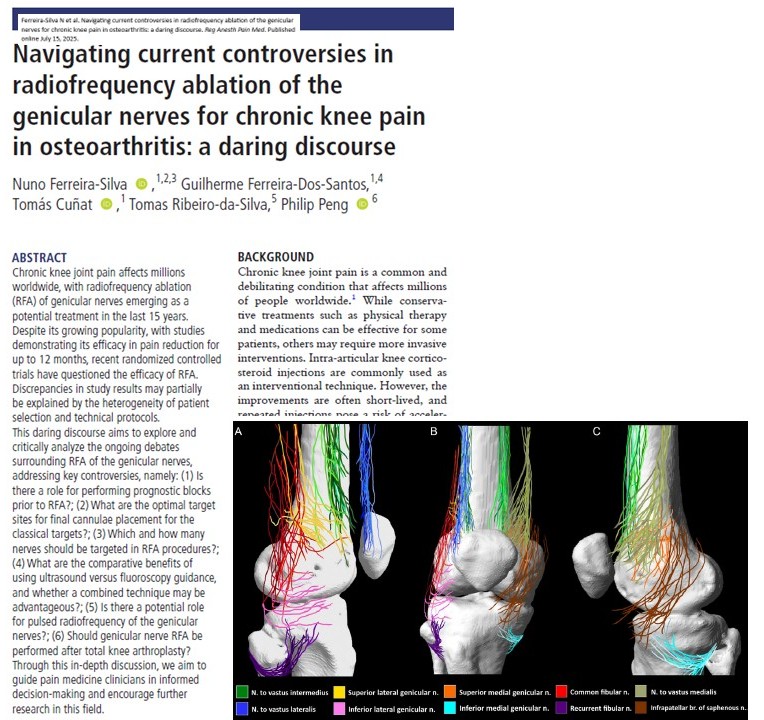
RFA is a minimally invasive procedure that uses heat generated by radio waves to ablate pain-transmitting genicular nerves around the knee joint.
Types of RFA:
- Traditional RFA: Uses standard electrodes and frequencies
- Cooled RFA: Reduces tissue charring, allowing for a larger lesion size
- Pulsed RFA: Delivers intermittent energy to avoid nerve destruction
RFA interrupts nociceptive input and can provide relief for 6 months or longer. It’s typically performed under fluoroscopic or ultrasound guidance.
Mesenchymal stem cell (MSC) injections
MSCs are multipotent stromal cells that can modulate inflammation, promote cartilage repair, and slow disease progression. They’re administered via intra-articular injection directly into the affected joint. Common sources include:
- Adipose tissue (ADMSC)
- Bone marrow (BMMSC)
- Umbilical cord blood (UBMSC)
MSC therapy is believed to provide longer-term benefits, potentially altering the disease course rather than merely addressing symptoms.
Study design and methodology
Objective
To compare the efficacy and safety of RFA and intra-articular MSC injections in managing knee OA symptoms.
Design
- Systematic review and network meta-analysis (NMA)
- Based on 34 randomized controlled trials (RCTs)
- Involved 2,371 patients across diverse settings
- Compared RFA and MSC therapies against:
- Placebo
- Corticosteroids (IACS)
- Hyaluronic acid (IAHA)
- PRP (IAPRP)
- Conservative therapy
Primary outcomes
- Pain scores at 3 and 6 months (measured via VAS or NRS)
- WOMAC scores (Western Ontario and McMaster Universities Osteoarthritis Index), assessing pain, stiffness, and function
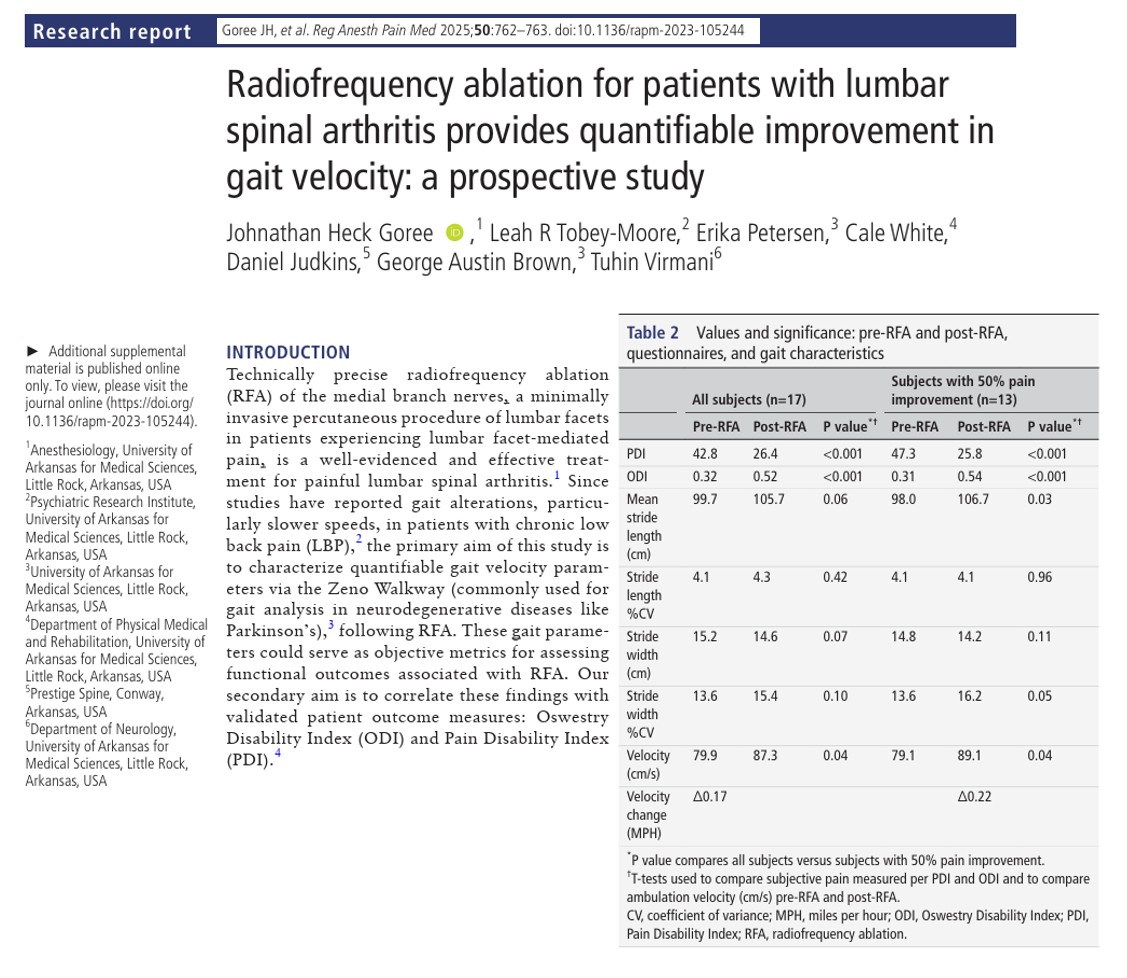
Key results
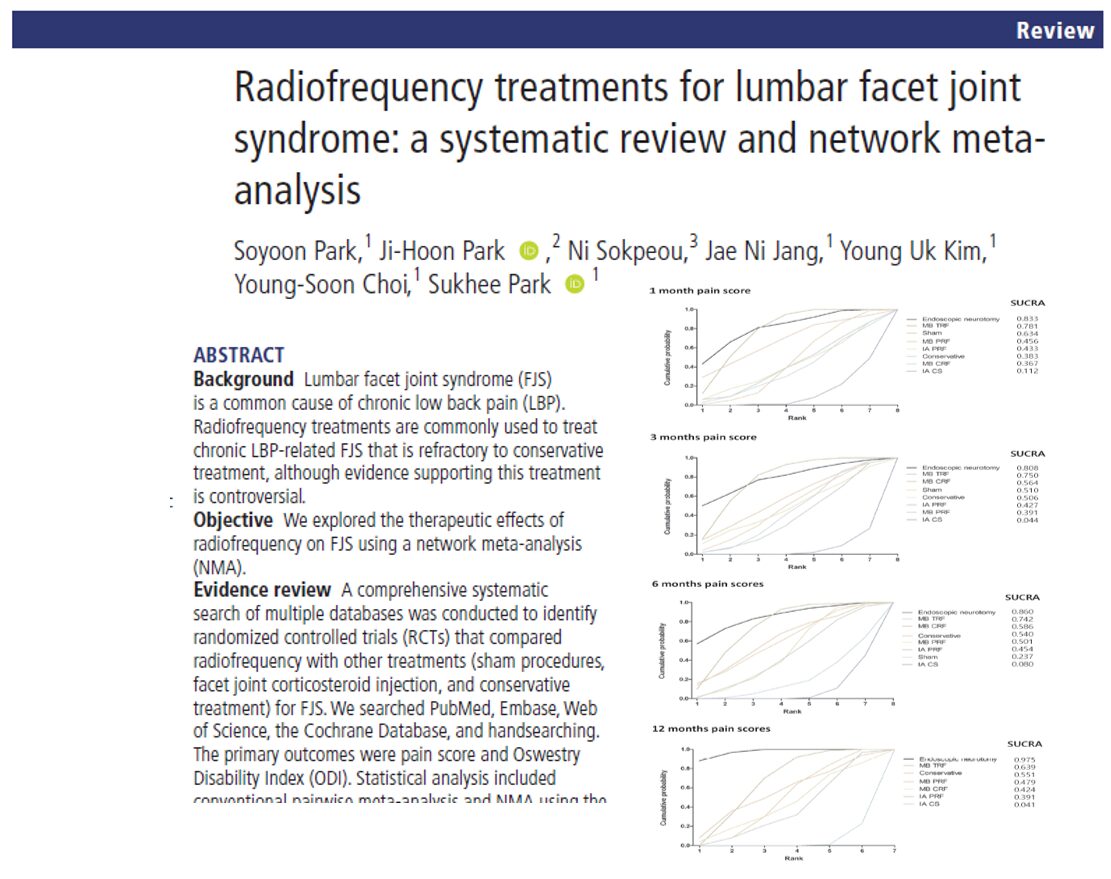
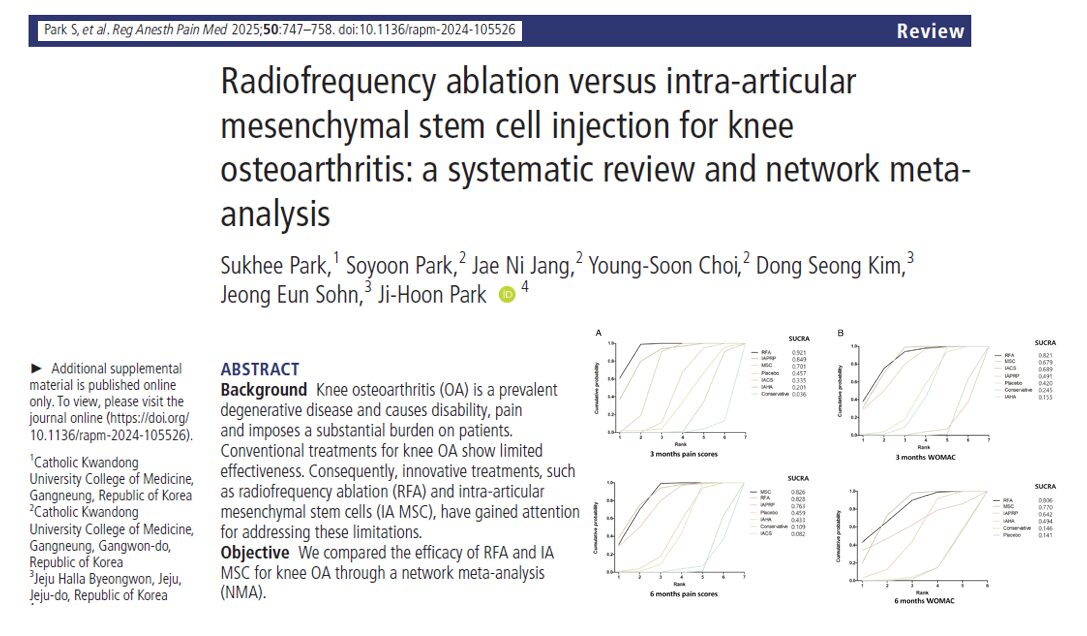
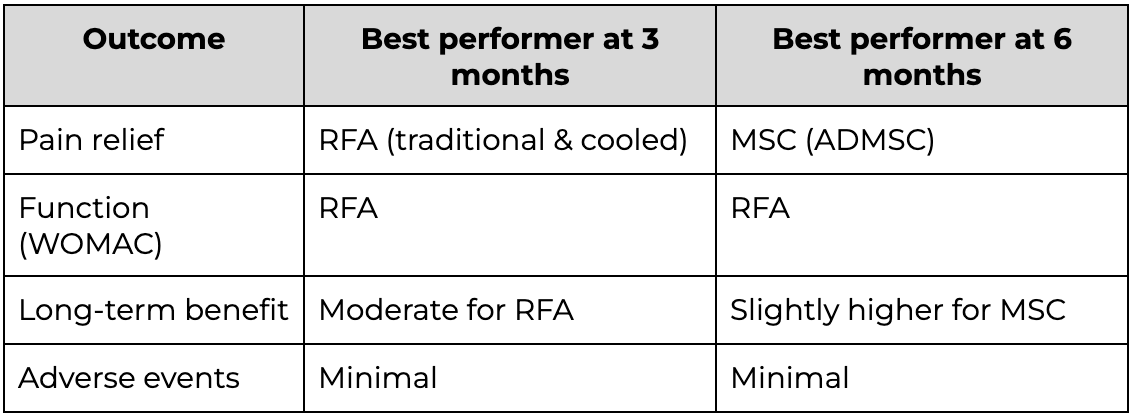
Pain scores at 3 months
- RFA ranked highest in pain reduction (SUCRA 0.921)
- MSC injections also significantly outperformed placebo, IAHA, and conservative treatment
- Traditional and cooled RFA, as well as ADMSC, demonstrated strong efficacy
Pain scores at 6 months
- MSC edged out RFA in long-term pain relief (SUCRA 0.828 vs 0.826)
- Both significantly outperformed IACS and conservative therapy
- ADMSC was especially effective, while UBMSC had moderate results
WOMAC scores at 3 months
- RFA showed superior improvements in joint function
- MSC injections, particularly BMMSC and ADMSC, were also effective
- RFA again ranked highest in overall effectiveness (SUCRA 0.821)
WOMAC scores at 6 months
Safety and adverse events
- RFA:
- Mostly mild side effects (e.g., transient injection site pain)
- Rare complications like skin burns or infection
- Minimal systemic risks
- MSC therapy:
- Transient joint swelling or pain in a minority of patients
- No serious adverse events linked to the injection itself
- Common side effects included bruising (especially with liposuction harvest)
- Both RFA and MSC outperformed placebo and conservative therapies
- RFA achieved slightly better outcomes than MSC (SUCRA 0.806 vs 0.770)
- Cooled RFA and BMMSC were top performers
Comparative summary of efficacy
How radiofrequency ablation is performed:
- Diagnostic evaluation and consent
- Local anesthesia and positioning
- Image-guided placement of electrodes
- Delivery of radiofrequency current to genicular nerves
- Recovery and follow-up within a few hours
How MSC therapy is administered:
- Donor cell preparation or liposuction (if autologous)
- Cell concentration and processing
- Intra-articular injection into the knee under sterile conditions
- Observation for 30–60 minutes post-injection
- Follow-up at 3–6 months intervals
Clinical implications
This landmark study provides evidence-based guidance for orthopedic surgeons, rheumatologists, and pain specialists treating knee OA.
- For short-term relief (3 months): RFA is highly effective and cost-efficient.
- For long-term regeneration: MSCs offer a disease-modifying approach.
- For patients unsuitable for surgery: Both options offer safer, non-surgical alternatives.
Treatment personalization, considering patient age, activity level, comorbidities, and preference, remains essential.
Study limitations
- Heterogeneity in treatment protocols (e.g., dosage, equipment)
- Short follow-up periods (most studies ≤12 months)
- Limited cost-effectiveness data
- Variability in MSC sourcing and preparation
- Need for longer-term RCTs comparing direct head-to-head outcomes
What’s next?
Future research should focus on:
- Long-term effects (12+ months)
- Optimal timing and frequency of treatment
- Head-to-head trials of RFA vs MSC (same patient groups)
- Economic evaluations and accessibility studies
Conclusion
Both radiofrequency ablation and mesenchymal stem cell injections show significant promise in treating knee osteoarthritis, offering effective and relatively safe alternatives to traditional therapies and surgery. RFA excels in immediate relief, while MSCs hold potential for structural regeneration and long-term benefit.
For clinicians and patients navigating the complexities of knee OA, these treatments offer hope, flexibility, and individualized options.
For more information, refer to the full article in RAPM.
Park S, Park S, Jang JN, et al. Radiofrequency ablation versus intra-articular mesenchymal stem cell injection for knee osteoarthritis: a systematic review and network meta-analysis. Regional Anesthesia & Pain Medicine 2025;50:747-758.
For step-by-step guidance on genicular nerve RFA and 50+ other techniques, read NYSORA’s Ultrasound-Guided Interventional Pain Manual. For the digital companion to this book, download NYSORA’s Ultrasound Pain App.