



Shoulder pain remains one of the most common musculoskeletal complaints encountered in both surgical and pain medicine practices. It affects millions of patients worldwide and is responsible for significant disability, reduced quality of life, and increased healthcare utilization. Advances in regional anesthesia and interventional pain management have highlighted the importance of targeted nerve interventions in managing shoulder pain.
Among the neural structures involved in shoulder innervation, the axillary nerve plays a crucial role. Historically, its significance in regional anesthesia has been underestimated relative to other nerves, such as the suprascapular nerve. However, emerging anatomical and interventional research demonstrates that the axillary nerve contributes substantially to both sensory and motor function of the shoulder joint.
Understanding the detailed anatomy, functional distribution, and imaging-guided approaches to this nerve is essential for anesthesiologists and pain physicians seeking to optimize perioperative analgesia and treat chronic shoulder pain.
The burden of shoulder pain in clinical practice
Shoulder pain ranks among the most frequent musculoskeletal complaints encountered in primary care and specialty clinics.
Epidemiological studies indicate that:
- Shoulder pain has a median global prevalence of approximately 16%.
- It is the third most common musculoskeletal presentation in clinical practice.
- Symptoms may range from mild discomfort to severe functional disability.
The condition often arises from multiple etiologies, including:
- Rotator cuff disease
- Glenohumeral joint pathology
- Subacromial bursitis
- Degenerative joint disease
- Post-surgical complications
In patients with moderate-to-severe symptoms, clinicians frequently employ advanced treatments such as regional nerve blocks, radiofrequency ablation, neuromodulation, or surgery.
Effective pain control is therefore essential not only for patient comfort but also for facilitating rehabilitation and improving surgical outcomes.
Complex innervation of the shoulder joint
The shoulder joint possesses one of the most intricate neural networks in the musculoskeletal system. Its innervation arises from several branches of the brachial plexus and surrounding cervical nerves.
Key nerves involved in shoulder innervation include:
- Suprascapular nerve
- Axillary nerve
- Lateral pectoral nerve
- Upper and lower subscapular nerves
These nerves supply both superficial and deep structures within the shoulder region.
Superficial sensory innervation
Cutaneous sensation over the shoulder originates primarily from:
- Supraclavicular nerves (C3–C4) from the cervical plexus
- Axillary nerve (C5–C6)
These nerves provide sensation to the skin covering the deltoid and surrounding shoulder area.
Deep articular innervation
The deeper structures of the shoulder, including the glenohumeral joint and acromioclavicular joint, receive articular innervation from multiple nerves.
Major contributions include:
- Suprascapular nerve
- Lateral pectoral nerve
- Subscapular nerves
- Axillary nerve
These nerves also supply ligaments and bursae surrounding the joint, contributing to both proprioception and nociception.
Interestingly, the axillary nerve innervates a large portion of the anteroinferior and posteroinferior glenohumeral joint capsule, highlighting its importance in shoulder pain pathways.
Anatomy of the axillary nerve
The axillary nerve originates from the posterior cord of the brachial plexus, typically carrying fibers from the C5 and C6 nerve roots.
From its origin, the nerve follows a complex course through the shoulder region.
Key anatomical pathway
The axillary nerve travels through several anatomical landmarks:
- Emerges from the posterior cord of the brachial plexus
- Passes between the pectoralis minor and serratus anterior muscles
- Travels along the anterior surface of the subscapularis muscle
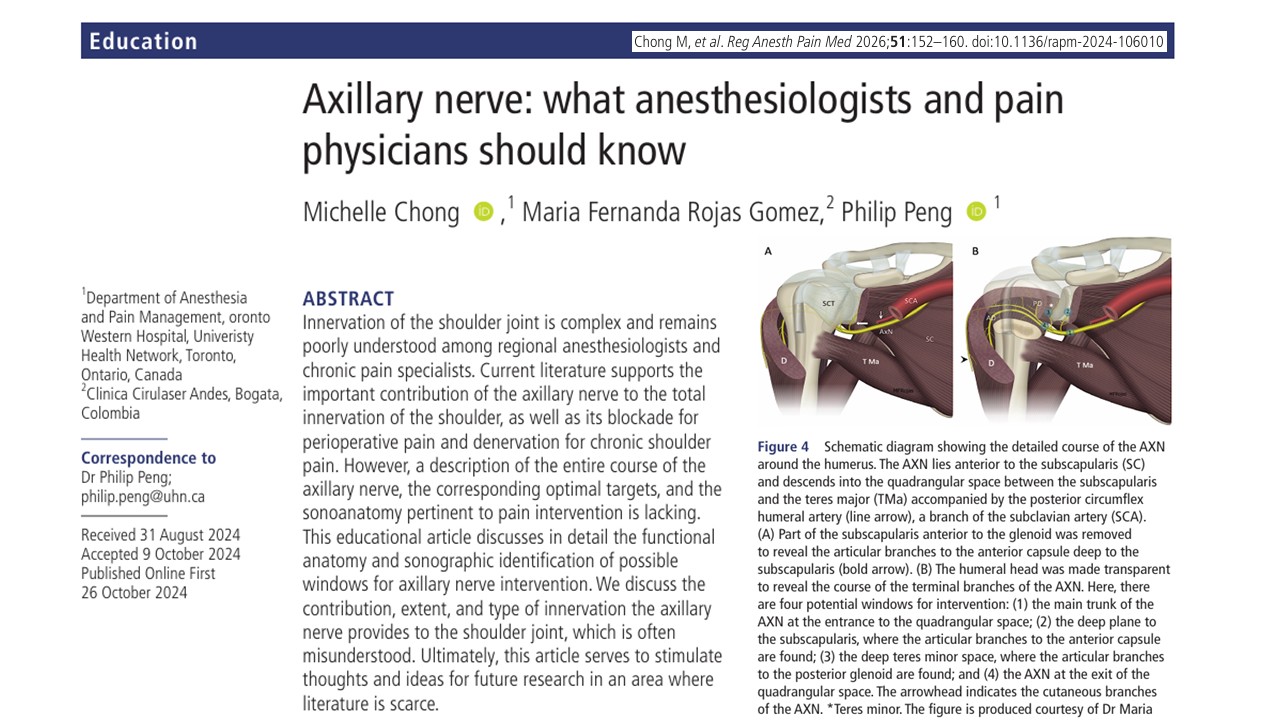
- Enters the quadrangular space alongside the posterior circumflex humoral artery
- Wraps around the surgical neck of the humerus
- Divides into anterior and posterior branches
This course allows the nerve to provide multiple motor, sensory, and articular branches.
Motor functions
The axillary nerve innervates two primary muscles:
- Deltoid muscle
- Teres minor muscle
These muscles are essential for:
- Shoulder abduction
- External rotation
- Stabilization of the glenohumeral joint
Damage to the axillary nerve can therefore produce weakness in shoulder abduction and impaired shoulder mobility.
Sensory distribution
The nerve also gives rise to the superior lateral cutaneous nerve of the arm, which supplies sensation to the skin overlying the deltoid region.
In addition, articular branches contribute to the sensory innervation of the shoulder joint capsule.
The quadrangular space: a critical anatomical landmark
A key anatomical structure associated with the axillary nerve is the quadrangular space.
This intermuscular space allows passage of the axillary nerve and the posterior circumflex humeral vessels.
Anatomical boundaries
The quadrangular space is bordered by:
- Superior: teres minor and subscapularis
- Inferior: teres major
- Medial: long head of the triceps
- lateral: surgical neck of the humerus
Within this space, the axillary nerve divides into anterior and posterior branches.
Understanding this region is vital for anesthesiologists performing nerve blocks and for surgeons working around the shoulder joint.
Functional role of the axillary nerve in shoulder pain
Research shows that the axillary nerve contributes significantly to the innervation of the shoulder joint.
The nerve supplies:
- The inferior capsule of the glenohumeral joint
- Portions of the subacromial bursa
- Surrounding ligaments and soft tissues
Importantly, different regions of the shoulder contain varying receptor types.
Nociceptive vs mechanoreceptive distribution
Studies demonstrate that:
- Nociceptors are concentrated in the upper half of the shoulder
- Mechanoreceptors dominate the lower half
The suprascapular and lateral pectoral nerves primarily supply nociceptor-rich regions, while the axillary nerve largely innervates mechanoreceptor-rich areas.
However, mechanoreceptors may still participate in pain transmission, particularly when sensitized by injury or inflammation.
This explains why axillary nerve interventions can provide meaningful analgesia.
Four key windows for axillary nerve intervention
Modern interventional pain practice identifies four potential anatomical windows for accessing the axillary nerve for therapeutic procedures.
These include:
- Entrance to the quadrangular space
- Deep subscapularis plane
- Deep teres minor space
- Posterior quadrangular space
Each window provides unique advantages and clinical applications.
First window: entrance to the quadrangular space
The first intervention point is the main trunk of the axillary nerve before it enters the quadrangular space.
characteristics
- Blocks sensory, motor, and articular branches simultaneously
- Located deep within the axilla
- The nerve lies superficial to the subscapularis muscle
Ultrasound imaging is typically required due to the depth and complexity of the surrounding anatomy.
A major limitation is that this approach often requires significant shoulder abduction, which may be difficult for patients experiencing severe pain.
Second window: deep plane to the subscapularis
The second intervention point lies in the deep plane between the subscapularis muscle and the anterior joint capsule.
This area contains articular branches from:
- Axillary nerve
- Nerves to the subscapularis
Clinical applications
Procedures performed in this plane may include:
- Diagnostic nerve blocks
- Radiofrequency ablation
- Cryoanalgesia
Small injection volumes can effectively reach the articular branches responsible for anterior shoulder pain.
Third window: deep teres minor space
The deep teres minor space provides access to articular branches from the posterior division of the axillary nerve.
Anatomical boundaries
This space is bordered by:
- Teres minor muscle
- Long head of the triceps
- Humeral neck
- Subscapularis muscle
Ultrasound imaging allows identification of this plane between the teres minor and the underlying joint capsule.
This region is particularly relevant for targeting pain arising from the posterior glenohumeral capsule.
The fourth window: posterior quadrangular space
The most commonly described technique for axillary nerve block targets the nerve after it exits the quadrangular space.
Advantages
- Relatively accessible with ultrasound
- Reliable identification using the posterior circumflex humeral artery as a landmark
- Can be performed with the patient seated or in the lateral position
Limitations
Because articular branches often leave the nerve earlier, this approach primarily affects:
- Motor branches to the deltoid
- Cutaneous sensory branches
Coverage of articular pain fibers may therefore be incomplete.
The role of axillary nerve blocks in shoulder surgery
Shoulder surgery frequently produces severe postoperative pain.
Approximately 45% of patients report significant pain immediately after surgery, emphasizing the need for effective analgesic strategies.
Current standard: interscalene block
The interscalene brachial plexus block remains the most widely used regional anesthesia technique for shoulder procedures.
However, this technique carries risks such as:
- Diaphragmatic paralysis
- Respiratory complications
- Phrenic nerve blockade
Alternative strategies
Combining suprascapular and axillary nerve blocks has emerged as a promising alternative.
Clinical studies show that this combination:
- Provides improved postoperative analgesia
- Reduces opioid consumption
- Lowers complication rates compared with the interscalene block
This approach may be particularly beneficial for patients with respiratory disease.
Axillary nerve interventions in chronic shoulder pain
Axillary nerve interventions are also gaining traction in the treatment of chronic shoulder pain.
Two emerging strategies include:
Radiofrequency ablation
Radiofrequency procedures target sensory branches supplying the shoulder joint.
These interventions aim to:
- Interrupt pain transmission
- Preserve motor function
- Provide long-term analgesia
Peripheral nerve stimulation
Peripheral nerve stimulation involves implanting electrodes near the axillary nerve. Electrical stimulation modulates neural signaling and can reduce chronic pain in selected patients. Early studies suggest promising results, although larger clinical trials are needed.
Future directions in shoulder pain management
Advances in anatomical understanding and ultrasound imaging are transforming the field of regional anesthesia.
Future research is expected to focus on:
- Improved imaging techniques for nerve visualization
- Optimized injection volumes and spread patterns
- Comparative studies between intervention windows
- Expanded use of neuromodulation therapies
Targeting articular branches rather than main nerve trunks may also improve analgesic outcomes while minimizing motor impairment.
Conclusion
The axillary nerve is a critical yet historically underappreciated contributor to shoulder innervation and pain transmission. Modern anatomical research highlights its significant role in both perioperative analgesia and chronic shoulder pain management.
Key points include:
- The axillary nerve supplies major motor, sensory, and articular structures of the shoulder
- Four anatomical windows provide potential targets for interventional procedures
- Combined suprascapular and axillary nerve blocks may improve postoperative pain control
- Emerging therapies such as radiofrequency ablation and peripheral nerve stimulation show promise for chronic pain treatment
For anesthesiologists and pain physicians, a thorough understanding of axillary nerve anatomy and imaging-guided techniques is essential for advancing patient care and improving outcomes in shoulder pain management.
As research continues to evolve, targeted axillary nerve interventions are likely to become an increasingly important component of multimodal shoulder pain therapy.
For more information, refer to the full article in RAPM.
Chong M, Rojas Gomez MF, Peng P. Axillary nerve: what anesthesiologists and pain physicians should know. Reg Anesth Pain Med. 2026 Feb 5;51(2):152-160.
Explore the axillary and suprascapular nerve block techniques in the NYSORA Nerve Blocks app. Prefer a physical copy? The bestselling NYSORA Nerve Blocks App is available in book format — an essential resource for mastering nerve blocks! And for a digital learning experience, check out the Nerve Blocks Module on NYSORA360!