Learn
Anesthesiology
Regional Anesthesia
Pain Management
IV Access
POCUS
Anesthesia Information for Patients
NYSORA360
Apps
Anesthesia
Nerve Blocks App
Anesthesia Assistant App
Pain Medicine
Ultrasound Pain App
Pain Medicine Assistant App
Imaging & Access
POCUS App
IV Access App
MSK Knee App
Veterinary
VetRA App
View all apps
Books
Regional Anesthesia
Nerve Block Manual
Regional Anesthesia Updates
Anesthesiology
Anesthesiology Manual
Anesthesiology Review
Anesthesia Updates 2025
Anesthesia Updates 2026
Pediatric Anesthesia Updates
Airway Management Updates
View all books & manuals
Pain Medicine
US Interventional Pain Manual
Pain Medicine Updates
Nursing
Mastering Difficult IV Access
PACU Nursing Manual
Veterinary
RA Veterinary Manual
Events
Conferences
Workshops
Boot Camps
View all events
News
Education
Industry
Media
Partners
Industry Marketing
Institutions
About
For Clinicians
Community
Fellowship
×
Learn
Anesthesiology
Regional Anesthesia
Pain Management
IV Access
POCUS
Anesthesia Information for Patients
NYSORA360
Apps
Nerve Blocks App
Anesthesia Assistant App
View all apps
Books
Events
Conferences
Workshops
Boot Camps
View all events
News
Education
Industry
Media
Partners
Industry Marketing
Institutions
About
For Clinicians
Community
Fellowship
Profile
Log In
POCUS
Midline shift
Cerebral vasospasm
Cerebral circulatory arrest
Intracranial hypertension
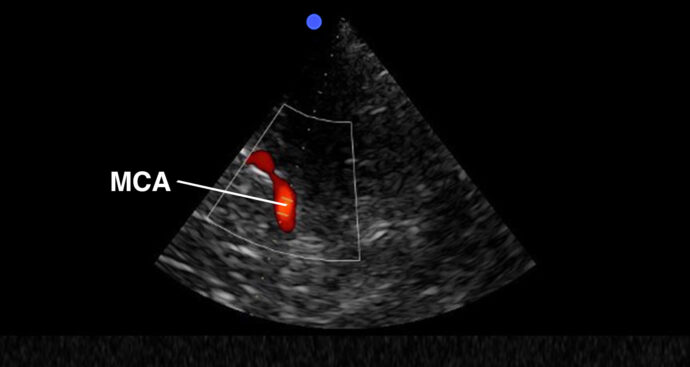
Essential transcranial Doppler
eFAST
Central venous catheter position – Rapid atrial swirl sign (RASS)
Basic valve assessment
Volume status assessment
Pericardial effusion – tamponade
1
2
3
...
>

 VetRA App
VetRA App

 VetRA App
VetRA App
 Nerve Blocks App
Nerve Blocks App Pain Medicine Assistant App
Pain Medicine Assistant App POCUS App
POCUS App IV Access App
IV Access App MSK Knee App
MSK Knee App Nerve Block Manual
Nerve Block Manual Regional Anesthesia Updates
Regional Anesthesia Updates Anesthesiology Manual
Anesthesiology Manual Anesthesiology Review
Anesthesiology Review Anesthesia Updates 2025
Anesthesia Updates 2025 Anesthesia Updates 2026
Anesthesia Updates 2026 Pediatric Anesthesia Updates
Pediatric Anesthesia Updates Airway Management Updates
Airway Management Updates US Interventional Pain Manual
US Interventional Pain Manual Pain Medicine Updates
Pain Medicine Updates Mastering Difficult IV Access
Mastering Difficult IV Access PACU Nursing Manual
PACU Nursing Manual RA Veterinary Manual
RA Veterinary Manual About
About