

Securing IV access in obese patients presents a unique set of challenges for healthcare professionals. The increasing prevalence of obesity worldwide has made this a common issue in clinical settings, necessitating a deeper understanding and specialized approaches to ensure effective venous cannulation. In obese individuals, the excessive adipose tissue can obscure superficial veins, making them difficult to palpate and visualize. This complicates the identification of suitable veins for cannulation and increases the risk of multiple cannulation attempts, leading to patient discomfort and potential complications such as hematoma, infection, or thrombophlebitis.
The anatomical and physiological alterations associated with obesity, including changes in blood vessel elasticity and the potential for deeper vein locations, require clinicians to adapt their techniques and equipment. For instance, using longer and larger gauge needles may be necessary to access deeper veins successfully. Additionally, advanced technologies such as ultrasound-guided IV access have become invaluable tools in overcoming the visualization challenges posed by obesity.
Given these complexities, healthcare providers must possess a high level of skill and patience, and understand the specific considerations and adaptations required for IV access in obese patients. This includes not only technical adjustments but also a compassionate approach that acknowledges the potential for increased anxiety and discomfort experienced by obese patients during venous cannulation. Addressing these challenges effectively is essential for delivering high-quality care and ensuring the safety and comfort of obese patients requiring IV therapy.

Examples of difficult veins in the hands of obese patients. The excessive adipose tissue obscures the veins.
Excess adipose tissue
- Challenge: Excess adipose tissue can obscure veins (e.g., veins on the dorsum of the hand and the deep brachial vein), complicating palpation and access.
- Solution: Ultrasound-guided IV insertion may be advantageous for identifying deeper veins and enhancing first-attempt success. Choose a longer catheter for proper vein access.
Diverse venous sites
- Challenge: Traditional venous access sites might be less feasible in obese patients.
- Solution: Explore alternative sites like the wrist’s inner side (i.e., volar aspect) and the cephalic vein between the deltoid and pectoral muscles. Prominent veins can often be found over the shoulders, upper torso, or breasts of obese patients. While not ideal for prolonged infusions, these sites can offer immediate, temporary access using a small-gauge IV. Following hydration, more conventional venous sites may become more accessible.

Alternative sites like the wrist’s inner side (i.e., volar aspect) can be used when traditional venous access sites are not feasible.


A) Prominent superficial chest veins are suitable for emergency cannulation in patients with difficult venous access in the upper or lower extremities. B) IV cannulation in the shoulder of an obese patient.
IV cannulation of a shoulder vein in an obese patient




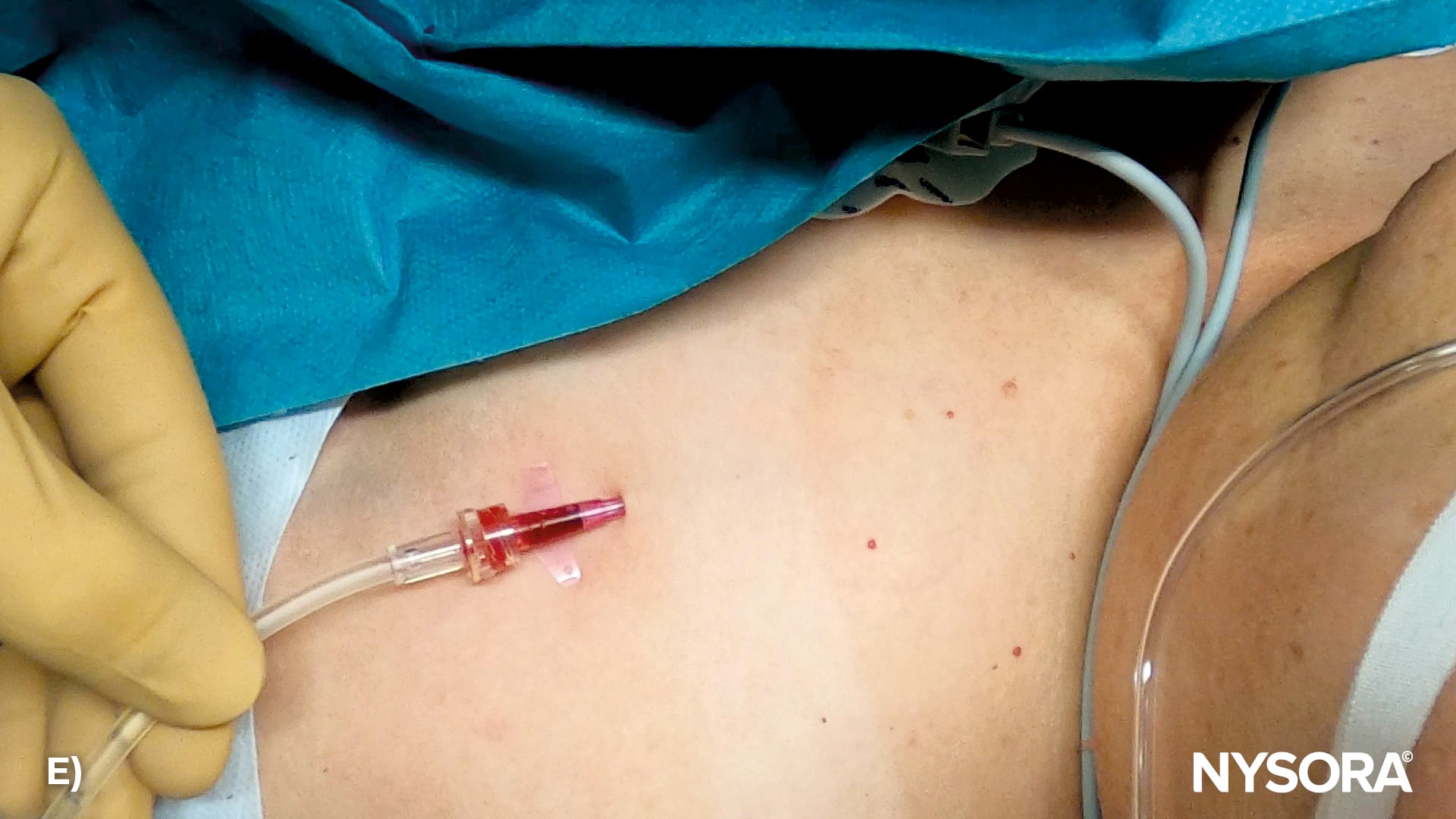
A) Example of a shoulder vein suitable for cannulation. B) Insert the needle at a shallow angle of 10 to 30 degrees relative to the skin. C) Appearance of blood in the flashback chamber. D) Thread the catheter over the needle into the vein, advance the needle-catheter system into the vein, and retract the needle. E) Attach the IV tubing to the catheter.
Venous access sites like the chest and shoulder veins should be reserved only for situations where other, more conventional sites are unavailable.
Risk of complications
- Challenge: The adipose tissue increases the likelihood of infiltration or extravasation of IV fluid.
- Solution: Frequently assess the IV site for early signs of infiltration and secure the catheter to reduce the chances of movement and displacement.
VIDEO: https://youtu.be/YipDrKFPzok











